In 1994, the Norwegian Association for Cardiothoracic Surgery established a countrywide register for all heart surgery in Norway. The register contains information about types of operation, risk factors, complications and 30-day mortality. In this article we discuss our experiences with the register and the importance of ownership and definitions, as well as a limited number of the variables registered and the significance of good feedback to specialist environments.
The Association resolved to establish a countrywide register for all heart surgery in Norway in 1992. The administrative committee for the register is formed by the Association?s quality and data committees. The articles of association and byelaws were adopted in 1993. Definitions of the variables registered are based on the database of the Society of Thoracic Surgeons (1) in the US and international consensus on how results are to be reported (2). This allows the comparison of Norwegian results with the results given in foreign registers. The database, which is owned by the Association, contains information on over 60 000 surgical operations on the heart and the large vessels in the vicinity of the heart. The Board is responsible for ensuring that the database is administered in accordance with the articles of association and byelaws. The register cooperates with the Norwegian Society of Cardiology, and every year a joint publication on open heart surgery and interventional treatment of coronary patients in Norway is produced (3). The Norwegian Register for Cardiac Surgery was one of the first to report data to the European Cardiac Surgical Register. Both registers are flexible regarding the choice of registration tools and can convert all ordinary data formats. The European Cardiac Surgical Register has so far issued four publications (4). The Norwegian Association for Cardiothoracic Surgery covers outgoing expenses for secretarial assistance, office equipment and specialist group meetings for the Norwegian register. The remaining tasks are covered by the honorary, unpaid work of office-holders. Previously the Association received a grant from the Norwegian Board of Health Supervision, but in recent years it has only received a grant from the Norwegian Medical Association?s quality assurance fund.
The register shows the considerable changes that have taken place during the period of registration from 1994 to 2008 (5). Coronary surgery remains the most frequently conducted type of operation with approximately 3 000 operations per year (fig 1). The largest increase is for aortic valve surgery and operations on the thoracic aorta. A growing number of operations are carried out both on elderly patients and new-born babies. There are major inexplicable differences between the counties with regard to the number of patients operated on per 100 000 individuals (fig 2) with a relatively large number of patients in the northernmost counties. Smoking habits, heavy work and a cold climate are factors that may explain this, but the database does not help to explain the considerable differences.
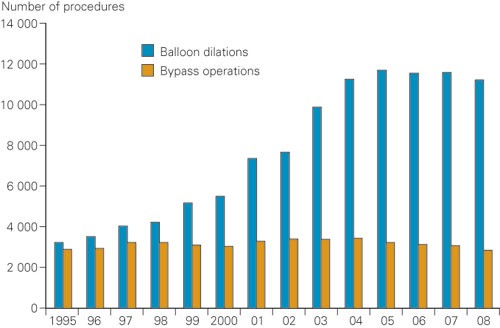
Figure 1 Development in coronary surgery and balloon dilation (PCI) 1995 – 2008
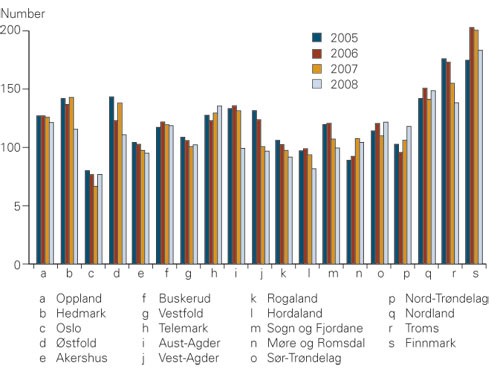
Figure 2 Distribution of all heart operations by county
The results compare favourably with the best results from foreign registers. The operation lethality (30-day mortality) for the most common type of surgery – coronary bypass surgery – is as low as 1.5??%. The results are also good for valvular heart surgery despite the large proportion of elderly patients. Mortality for children?s heart surgery has decreased gradually, in line with what we have observed in Sweden (6).
Ownership
There are seven large public medical registers in Norway. These are given legal authority by the Personal Health Data Filing System Act of 18 May 2001. Each of these registers has its own statutory provisions. In addition there are 50 medical quality registers (7). Like several other medical quality registers, our register is based on the quality work undertaken by the Norwegian Medical Association. The Norwegian Board of Health Supervision has expressed doubts as to whether the specialist associations under the Norwegian Medical Association can act as the legal owners of a register (8). Of the approximately 50 medical quality registers in the somatic specialist health services described in the report of the Directorate of Health and Social Affairs of March 2004 (9), as many as 36 are so comprehensive that the Directorate considers that they can be designated national registers. The working group which drew up the report recommends that 15 of these registers, including the Norwegian Register for Cardiac Surgery, should be upgraded as national medical quality registers, and that joint electronic solutions should be developed for feedback to the reporting departments, comparison of data and publication. Furthermore, the working group recommends that each regional health enterprise should be responsible for the data processing of selected quality registers and thus be in charge of the professional adaptation and administration/technical operation.
In our opinion the specialist associations under the Norwegian Medical Association should continue to own and run the medical quality databases. Public medical registers are based on diagnosis and treatment codes that are registered when the patient is discharged (10). Our view is that it is difficult to base registration of risk factors and complications on ICD- and procedure codes alone. Traditionally, medical quality registers have collected data by using registration forms or the data files submitted. A few databases have now started to use web-based online registration (11). It has been demonstrated that medical quality registers can result in improved quality in treatment (12), and data from the register can be used in health research and in making political decisions. Our type of register may be vulnerable because it demands local competence, enthusiasm and willingness to carry out voluntary, unpaid registration work. This not only applies to the secretariat functions but also to the work that is carried out in the cardiothoracic centres. Nevertheless, we believe that ownership of a register has a great effect on its quality. We have found that there is a strong sense of loyalty to the register regarding completeness and data quality, and we fear that data quality will be reduced if a requirement to register data with a regional health enterprise is introduced. The external monitoring of data (an audit) is desirable but would demand greater resources that those offered by the Norwegian Association for Cardiothoracic Surgery today. We feel that such quality assurance of data can best be conducted by the quality assurance committees of the specialist associations with funding provided by the Norwegian Medical Association.
Reporting and publication
All the centres are sent an overview of their own data and results, as well as a countrywide overview. The total figures for the entire country are published on the websites of the hospitals or of the Medical Association (5). The central register form can be found here.
The information on the database is de-identified. The Data Inspectorate has not given permission for the registration of the patient’s identity unless each patient has given his/her informed consent. Such consent will not generally be possible because a large proportion of the patients are hospitalized with reduced consciousness (cardiogenic shock, hypovolemic shock secondary to rupture of aneurysms etc). Substantial differences among hospitals when it comes to the patient profile, the type of operation and the length of stay make it difficult to compare results (for example operation mortality and postoperative complications). Data from the Norwegian Register for Cardiac Surgery show that up to half of the patients who die within 30 days of an operation die after being discharged from the hospital department. Therefore it is important that the individual hospitals do not merely register deaths in the hospital.
There are methods of measuring the total treatment and care requirement in the field of heart surgery. All seven cardiothoracic centres within heart surgery in Norway have adopted EuroSCORE, a scoring system that predicts the anticipated risk in relation to a heart operation (13), based on risk factors and the type of operation.
So far not all hospitals have said they are willing to publish their own results, even though the time seems to be ripe for this (14). Since the register does not identify patients, we cannot conduct long-term survival studies. Moreover, a wide-ranging comprehensive analysis of medical quality registers reveals that few registers include treatment costs (15). Nor does our register permit the calculation of costs linked to individual procedures. Compared with the European register and the American STS-database, the results achieved by Norwegian cardiothoracic surgery are good. However, Norwegian heart-operated patients are no older and no more ill than patients in Central Europe. The number of women who are operated on is low, and this also applies to the proportion of operated patients suffering from obesity and diabetes mellitus (4). The percentage of emergency operations is as expected. Operation mortality has not increased despite the fact that patients are older and to some extent also in need of a greater degree of treatment and care. This may indicate that the quality of heart surgery in Norway is continually improving.
Conclusion
The Norwegian Register for Cardiac Surgery is now entering its 15th year. All seven departments report all operations and the register data are presented on the Medical Association’s website and on the websites of the individual hospitals. The members of the Medical Association can freely extract and make use of the information presented. Moreover, the Norwegian Association for Cardiothoracic Surgery experiences a growing interest in the yearly reports. The register has now assumed its final shape and there are no plans for major changes or extensions.
Appendix
