2010 was the 200th anniversary of Chopin’s birth. Frédéric François Chopin, christened Fryderyk Franciszek Chopin, was born in Żelazowa Wola, a small town near Warsaw. The date of birth has not been definitely established. A birth certificate has been found that gives the date 22 February 1810 (1, 2), but Chopin himself always gave his date of birth as 1 March. He died on 17 October 1849 in Paris, 39 years old.
Chopin’s musical talent was apparent early. He was considered as a child prodigy and started to compose when he was only seven years old (3, 4). The first polonaises in B major and G minor are dated 1817 and show an unusual talent for improvisation. From 1822 he received private tuition in music theory and composition. He took the secondary school examination in 1826 and then studied at the conservatory, first counterpoint, and then theory of music, basso continuo and composition (3, 5). He also attended lectures at the university.
When he was 20 years old Chopin left Warsaw and travelled to Vienna. Shortly afterwards, the Polish November uprising broke out. The subsequent oppression by Russia made it difficult to return to Warsaw, although he longed to go home, and wanted to support the insurgence (1, 3, 6). His father advised him against returning and thought that he could serve his country better with his music than with a gun (2, 3, 5). Torn between anxiety for his family and his dream of fame in the world of music, he chose to go to Paris, where he spent most of his life.
In Paris he found a creative environment and a circle of acquaintances that included many of the best known authors and composers of the time (5). He managed well socially and financially and made a living as a piano teacher, composer and concert pianist. Although he was an ardent Polish patriot (2, 3), he used the French version of his name, by which he is best known.
Chopin is one of the most influential and popular composers of piano music of the 19th century. In Poland he is regarded as the person who has had most influence on the country’s history of music (3, 7). Chopin composed almost exclusively for piano solo and has been called the pianists’ composer. He was a brilliant pianist and his music was primarily an expression of poetry, emotion, depth and delicate nuances. More than 230 of his compositions have been preserved, only a few manuscripts and pieces from early childhood have been lost. There is a total of about 80 opus numbers. The piano is present in all of them, and most of them are for solo piano. In spite of poor health and a short life, his works include 27 etudes, 26 preludes, 21 nocturnes, 58 mazurkas, 17 polonaises, 19 waltzes, 4 impromptus, 2 concertos, 4 ballades, 4 scherzos, and 3 sonatas as well as several other pieces (7).
Several other well-known composers such as Wolfgang Amadeus Mozart (1756 – 91), Franz Schubert (1797 – 1828) and Felix Mendelssohn (1809 – 47) also died before they were 40 years old. However, these composers died rather suddenly and unexpectedly whereas Chopin had poor health for most of his adult life (fig. 1).
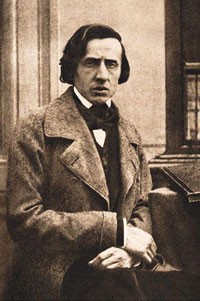
Figure 1 The only known photograph of Chopin, 38 years old
Medical history of Chopin’s family
Chopin’s father suffered to some extent from respiratory tract infections, but lived until he was 73 years old. His mother had good health and died aged 77 (6, 8, 9). Chopin had three sisters. Isabella died aged 70. Ludwika suffered extensively from respiratory tract infections and allegedly died of a lung disease aged 47. Emilia was a vivacious child with poor health. She suffered from recurrent respiratory tract infections, dyspnoea, loss of weight and haematemesis, and died after a massive upper gastrointestinal haemorrhage only 14 years old (5, 6, 9).
Chopin’s chronic symptoms
During his teens, Chopin had frequent respiratory problems, diarrhoea and loss of weight (6). In 1826, 16 years old, he had a period of six months with symptoms including cough, headache, and swelling of the cervical lymph glands (3, 6). He had similar symptoms while living in Vienna as a 20 year-old (10, 11). Many episodes of bronchitis and laryngitis are described during the period from 1831 to 1835. He never developed proper facial hair or beard, and although it is thought that he had sexual relations with several women, he never fathered any children (11, 12).
During an epidemic of influenza in Paris in 1837, Chopin developed high fever, haemoptysis and haematemesis. His doctor, Dr Paul-Léon-Marie Gaubert (1805 – 66), considered that he did not suffer from tuberculosis and recommended a warmer climate (6). It has been speculated whether this physician really thought that he did not have tuberculosis, or whether he chose a different diagnosis to avoid possible stigmatisation of a patient with this disease (6). Chopin was constantly troubled by dyspnoea and tired easily. He often had to be carried to bed after having played the piano for a long time.
In 1836 he met the author Aurore Dudevant (1804 – 76), better known as George Sand. In November 1838 he accompanied her and her two children to Mallorca to escape the winter (3, 6, 8). The journey did not have a good effect on his health. In Valldemossa (fig. 2) he was constantly troubled by fever, cough and diarrhoea. In spite of this he was productive. The 24 preludes (opus 28 found its’ final form during the stay in Mallorca. The doctors he consulted there considered that he had tuberculosis (8, 10). The local population therefore avoided him for fear of being infected. George Sand had to pay for his furniture to be burnt when they left Valldemossa (3, 6, 8). In February 1839 they returned to the mainland and spent some time in George Sand’s country house Nohant, but they moved back to Paris during the autumn. From 1840, Chopin’s health condition deteriorated. He lost still more weight (weighing only 45 kilograms) and was described as pale, thin, and looking ill (6). A caricature drawn by a friend in 1844 clearly shows that he had developed a barrel chest (6, 13).

Figure 2 The town Valldemossa on Mallorca, where Frédéric Chopin and George Sand spent the winter of 1838 – 39. Photo Istockphoto
Chopin had several periods of depression (3). He complained of depression, hopelessness, apathy and sleeplessness during his stay in Vienna in 1830 – 31 (3), probably as a reaction to the uprising in Poland and his doubts about moving to France. Later in his life, his episodes of depression seem to be related to exacerbations of his disease (3). It can therefore be speculated whether his mental health was an expression or a consequence of a progressive chronic disease with severe symptoms or whether he suffered from a primary mental disorder.
The last years
He experienced a better period during the winter of 1847. Although he was still short of breath and lacked energy, he decided to travel to London (2, 4). He had hoped to perform in a series of concerts, but was confined to bed for most of the time. However, in April 1848 he felt well enough to go to Scotland at the invitation of Jane Stirling (1804 – 59). She was a previous pupil who had looked after Chopin following the break with George Sand. Although he managed to perform in concerts in Edinburgh, Manchester and Glasgow, he was usually so exhausted that he had to be carried upstairs to his bedroom (3, 6). Once back in London he was confined to bed with fever, cough and a feeling of suffocation. He therefore decided to return to Paris on 19 November.
His condition then rapidly deteriorated. In addition to cough, dyspnoea and fluctuating fever, he suffered from painful wrists and ankles, haemoptysis, haematemesis and ankle oedema (3, 6, 10). Several doctors were consulted and gave different assessments and advice. Nevertheless, they all agreed that he was too ill to be able to move away from Paris (6, 10).
His last days
At the beginning of October 1849, the situation deteriorated further. Chopin was no longer able to sit up and he was so weak that he could only whisper (11). At times he was considered to be unconscious. He was visited by his sister Ludwika, and told her that he wanted his heart to be taken to Warsaw after his death, and that Mozart’s Requiem in D minor should be played at his funeral (4, 7). He died at 2 a.m. on the morning of 17 October 1849 after having been unconscious for 24 hours. On the same day, Jean Baptiste Auguste Clésinger (1814 – 83) made a death mask (fig. 3) and a plaster cast of his hands (3, 6). The diagnosis written in the death certificate is tuberculosis in the lungs and larynx (6).
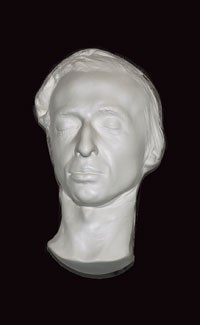
Figure 3 Chopin’s death mask
The funeral took place on Tuesday 2 November in the Madeleine church in Paris. As Chopin had asked for Mozart’s Requiem, the funeral was postponed for two weeks. This was because female singers (in addition to choir voices there are solo parts for contralto and soprano) were not allowed in this church. However, the rule was relaxed in the end on condition that the female singers were placed behind a screen (2, 7, 14). Chopin’s own preludes number 4 in E minor and number 6 in B minor were also performed. Frédéric Chopin was laid to rest in the Père-Lachaise churchyard in Paris. In accordance with his wish, his heart was taken to Poland and placed in an urn in The Holy Cross Church in Warsaw.
Autopsy
The autopsy was carried out by Dr Jean Cruveilhier (1791 – 1874) (6, 15). He was considered to be one of the most prominent medical authorities of the day and was Professor of Surgery, Anatomy and Pathology (16). He wrote several books on tuberculosis (16). The autopsy report has never been found. According to Jane Stirling, in correspondence with Franz Liszt Professor Cruveilhier stated that «the autopsy gave no answer as to the cause of death, but the lungs were less affected than the heart. This is a disease that I have not seen before.» (8, 17).
Differential diagnoses
Tuberculosis
Tuberculosis has existed for several thousand years. The prevalence of the disease reached a peak in the 18th and 19th centuries (8, 18). Almost half the population of England probably had some form of active tuberculosis during the first half of the 20th century (8). The first modern clinical description of the disease was published in 1810 (18). The tubercle bacillus, however, was first demonstrated in 1882.
In the 19th century, treatment of pulmonary tuberculosis consisted of rest, good nourishment and strengthening of the body’s own defence mechanisms (18). This usually took place in separate sanatoria, which also acted as isolation institutions for infectious people. It was thus a prevalent disease when Chopin was alive. He could have been infected during his youth by his sister Emilia. She may have died of tuberculosis, but this does not give a good explanation of her gastrointestinal haemorrhages. If Emilia had suffered from miliary tuberculosis or direct progression of a primary lesion, her symptoms would probably have been more dramatic, given her very young age (15). However, none of the other members of the family had obvious signs of tuberculosis (15).
Chopin’s haemoptysis can be explained by the disease, but lack of finger clubbing and his haematemesis and diarrhoea point towards another diagnosis. Although Cruveilhier’s autopsy report has never been found, second-hand reports indicate that he was convinced that Chopin suffered from another disease (8, 10, 17). If the composer really had tuberculosis, it is conspicuous that he did not infect those in his immediate surroundings – such as George Sand and her two children – in the course of a long period of exposure (8).
Cystic fibrosis
Cystic fibrosis is a hereditary congenital disease affecting the glandular function of several organs including the lungs, gastrointestinal tract and pancreas (19). Those affected have abnormal respiratory secretion and diminished local mucous membrane defence in the airways. This predisposes to colonisation and infection by different microbes that seldom cause disease in healthy individuals. Most patients need frequent and prolonged treatment with antibiotics for bacterial infections and colonisation in the airways.
Cystic fibrosis is the commonest known autosomal recessive hereditary disease (19). During the period before antibiotics, patients seldom lived until they were 30 years old. However, there are different degrees of severity of this disease and it cannot be ruled out that Chopin had a mild form (12). The condition is associated with recurrent episodes of pneumonia, pancreas deficiency, liver cirrhosis and infertility. This fits in with the fact that Chopin had no children, and with his diarrhoea, which was possibly caused by pancreas insufficiency with fat intolerance and steatorrhoea (8).
Alpha-1-antitrypsin deficiency
This is a codominant hereditary disease where the alpha-antitrypsin level in the blood is too low. There are various genetic variants, but among those who develop the disease, 95 % have a deficiency of what is termed the Z gene (or Z allele) (9, 13). Some genetic variants predispose primarily for liver disease, others for lung disease and some for both conditions (9, 20). The symptoms of alpha-1-antitrypsin deficiency include dyspnoea, recurrent respiratory tract infection or obstructive asthma with poor response to normal treatment. Those affected may develop pulmonary emphysema at the age of 30 to 40 years. The disease may also lead to impaired liver function in some patients and liver lesions are very common. Some patients develop cirrhosis and liver failure (6).
Alpha-1-antitrypsin deficiency could explain Emilie’s death at the age of 14 of haematemesis, possibly caused by oesophageal varices due to portal hypertension (9). It is true that one might have expected concurrent icterus or ascites, but these findings have not been described (8, 9). Alpha-1-antitrypsin deficiency could explain Chopin’s recurrent pulmonary infections, loss of weight and gastrointestinal symptoms. He suffered from these symptoms throughout his whole adult life.
Diagnosis and pathography
It is possible that Chopin suffered from the same disease as his sister Emilia, and likely that his doctors were uncertain about the condition. In several articles, various differential diagnoses have been discussed (3, 6, 21 – 23), and at present there is no absolute agreement on the cause of death.
Articles dealing with diseases in deceased famous people are often called pathographies (24, 25). A pathography may be written as a testimony of the disease, almost a travelogue describing the experiences of the author in a new and unaccustomed landscape (25). Differential diagnoses may be interesting, but are often speculative and assessed on the background of observations made by others in a non-medical context. This means that it is completely impossible to test a hypothesis about which disease was really present.
However, in the case of Chopin we possess organic material that could theoretically be tested against some of the relevant differential diagnoses. Chopin’s heart is at present in a crystal urn filled with alcohol, brought back from Paris by his older sister Ludwika in 1849 and stored in The Holy Cross Church in Warsaw. With today’s gene technology, it might be possible to discover whether he suffered from cystic fibrosis or alpha-1-antitrypsin deficiency. Dr Michal Witt from the Institute of Molecular and Cellular Biology in Warsaw has applied for permission to carry out genetic tests on Chopin’s heart (12). However, a spokeswoman from the Polish Ministry of Culture, Iwona Radziszewska, stated on 21 July 2008 that it had been decided that permission would not be given to carry out these tests (26).
Conclusion
In spite of his debilitating disease, Chopin was musically creative, even during periods with deterioration of his symptoms. We will probably never discover the cause of death. The most likely differential diagnoses are tuberculosis, cystic fibrosis or alpha-1-antitrypsin deficiency. Is it important to know what Chopin died of in order to enjoy his music?
Of course not!
Many composers admired and found inspiration in Chopin’s music (3, 27). The rest of us can also be inspired by a composer and brilliant pianist who, in spite of a serious disease and suffering for most of his short life, worked so hard and produced such fantastic piano compositions.
On the other hand, it is interesting to make medical speculations about how so many years of suffering might have influenced Chopin as a composer and performing artist. He was not a pianist for large concert halls and preferred small salons (27, 28). His touch could lack power (10), and he preferred short compositions (7, 11, 28). This could be related to his physical limitations, but could of course also be an expression of a deliberate piano technique and musical expression. The episodes of depression may have been secondary to exacerbation of the disease, but a primary mental disorder cannot be excluded (3, 11). Nevertheless, it is striking that the years between 1839 and 1846 were his most creative period, and coincided with deterioration of his condition (3).
In conclusion we can reasonably conclude that Chopin’s illness must have influenced his musical expression, which is characterised by intimacy, melancholia and sentimentality (7).
