Norwegian legislation refers to two types of autopsies: forensic post mortem, which is undertaken at the request of the police, and clinical autopsy, in Norway called hospital autopsy, which is undertaken for medical reasons (1, 2). The 1973 Act relating to hospital autopsies was drawn up at a time when most people died in hospital (3). Today, the majority of all deaths occur in nursing or health institutions, and the application of the Act has changed accordingly (4). The notes to the new regulations for the Act, issued in 2004, specify that it now also applies to those who die outside institutions, for example in their own homes, and the social insurance system covers the cost of transport of the deceased to and from the department of pathology as well as the examination (5 – 7). A recently submitted proposal for new autopsy legislation suggests a change of nomenclature in line with the change in place of death, using the term «medical autopsy» instead of «hospital autopsy» (8). The committee proposes that this term should be used for all non-forensic autopsies, irrespective of whether these are performed on those who die while in hospital or elsewhere (referred to as outpatient autopsies).
Deaths outside hospital are rarely subjected to further investigation to clarify the cause of death. Often, there can be doubts as to whether they should be regarded as following from natural or unnatural causes (Box 1) (9). In our experience, not everybody is aware of the opportunity to obtain a clarification of the cause of death with the aid of a medical autopsy if the police do not request a forensic post mortem. The recently submitted legislative proposition proposes a general obligation for doctors to assess the need for an autopsy, irrespective of place of death (8). If the proposition is adopted, one would expect an increase in the number of medical autopsies performed after deaths outside hospital. However, nothing has so far been published to describe what kinds of deaths are currently investigated by way of a medical autopsy in Norwegian departments of pathology. We therefore present an overview of those deaths that have been investigated by the Department of Pathology at Akershus University Hospital during the last five years. In the following, the studied group of autopsies will be referred to as medical autopsies of deaths outside hospital.
BOX 1
A death is regarded as unnatural if it may have been caused by: (9)
Homicide or other bodily harm
Suicide or self-inflicted injury
Accidents such as shipwreck, fire, landslide, lightning, drowning, fall, traffic accident or similar
Industrial accident or industrial injury
Error, negligence or accident in examination or treatment of an illness or injury
Substance abuse
Sudden and unexpected death of an unknown cause
The following are also reported as unnatural:
Material and method
All medical autopsy records of deaths outside the hospital were identified by a manual search through the autopsy records at Akershus University Hospital for the period 2007 – 2011. Deaths that occurred in the ambulance on the way to hospital were not included, even though the patient was not registered as admitted. Data were registered only from autopsy records. The following information was noted: gender, age, type of requisitioning agent, time of death (first or second half of the year), mode of death (found dead in or outside the home or in an institution, observed death, accident, suspected suicide) and other relevant information about the death (known somatic disease, recent medical attention, psychiatric patient, known substance abuse). The autopsy results were translated into ICD-10 codes (International Classification of Diseases, version 10) (10). Forensic toxicological examination and its contribution to assessment of the cause of death were also registered. Information on the number of medical autopsies of deaths outside hospital for the years 2007 – 2010 for the country as a whole was retrieved from the Cause of Death Registry.
The study was characterised as a quality assurance study, and was approved by the data protection officer at Akershus University Hospital.
Results
In the course of five years, a total of 89 medical autopsies were performed at the Department of Pathology, Akershus University Hospital, of patients who had died outside hospital. Among the deceased, there was a majority of men (60 deaths), and they were significantly younger than the women (the median age of men and women was 58.5 and 65 years respectively). The annual number of autopsies increased consistently over the five-year period – from 13 in 2007 to 26 in 2011 (Figure 1). With the exception of 2008, the number peaked in the last half of the year (Figure 2). The number of medical autopsies after deaths outside hospital submitted to the Cause of Death Registry for the country as a whole has increased by 45 % from 2007, from 150 in 2007 to 218 in 2010.
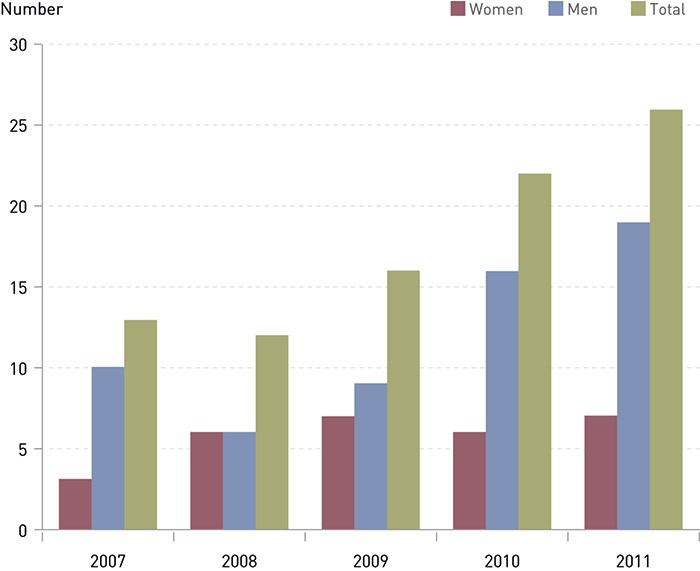
Figure 1 Medical autopsies of deaths outside hospital in Akershus University Hospital during the period 2007 – 2011. Gender distribution and the number of deaths (N = 89).
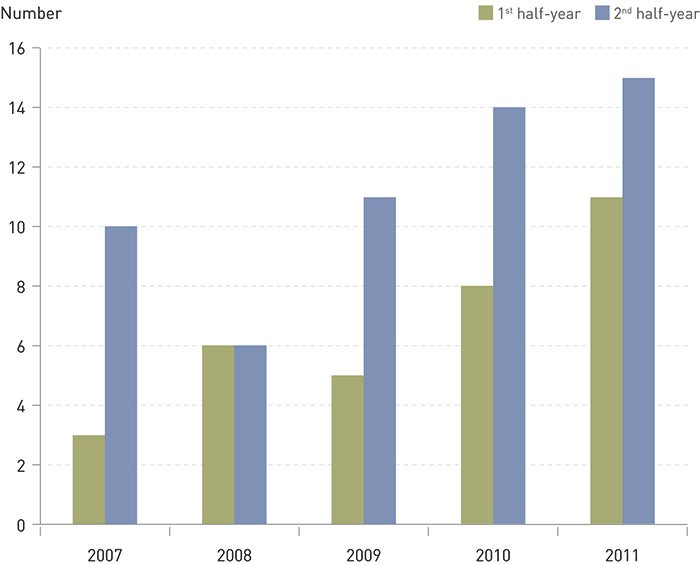
Figure 2 Medical autopsies of deaths outside hospital in Akershus University Hospital during the period 2007 – 2011. Distribution by first and second half of the year. (N = 89).
The circumstances surrounding the deaths and the clinical information in the autopsy requests examined at Akershus University Hospital are summarised in Tables 1 and 2. Most of the deceased had been found in their own home or in their holiday home, and suffered from known somatic diseases. In the case of deaths that had occurred immediately after medical treatment had been initiated, uncertainty regarding the treatment was often a cause for an autopsy request. For 35 of the deaths, no previous illness was reported. The proportion of deceased persons with no known previous history was largest in the group of observed acute deaths (11 of 18) and among those who were found in their home or holiday home (17 of 53).
|
Table 1 Circumstances around the deaths for autopsies performed at Akershus University Hospital of deaths outside hospital during the period 2007 – 2011
|
|
Circumstances
|
Number
|
|
Found dead at home or in holiday home
|
53
|
|
Observed death, at home or outside
|
18
|
|
Died in nursing home/other institution
|
10
|
|
Found dead outside
|
4
|
|
Accident or assumed suicide
|
4
|
|
Total
|
89
|
|
Table 2 Clinical information for medical autopsies performed at Akershus University Hospital on patients who died outside hospital in the period 2007 – 2011
|
|
Clinical information
|
Number
|
|
No reported medical history
|
35
|
|
Known somatic disease
|
19
|
|
Abuse of alcohol or other substances
|
15
|
|
Under treatment for acute illness
|
14
|
|
Known mental disorder (not substance-related)
|
6
|
|
Total
|
89
|
According to the requests, evidence of unnatural death was present in four cases. These included accidents or assumed suicides that were not forensically examined, and therefore had been referred to a medical autopsy by GPs or emergency doctors. Whether the police had been called or the case had been reported as an unnatural death were not systematically reported in the autopsy records for the remaining cases. Deaths that had occurred without any witnesses, where the deceased had no known previous medical history, was known to abuse substances or where there was a possible correlation with medical treatment must all be considered as unnatural, however, so that the circumstances summarised in Table 1 indicate that the majority of the deaths would most likely comply with the legal definition of unnatural death.
Altogether 82 % of the cases were requested by a GP or an emergency doctor (34 and 39 requests respectively). The remaining autopsies had been requested by supervisory doctors (nine requests), a public medical officer (two requests) or hospital doctors at Akershus University Hospital (five requests).
In 75 of the 89 cases a natural cause was found. In three cases, the cause of death remained unclear, and in 11 cases the cause of death was unnatural – a result of external causes, such as an accident or an unintentional or intentional self-inflicted injury. The underlying causes of death after the autopsies are summarised in Table 3. Cardiovascular diseases were the most frequent cause of death. This cause of death was especially prominent in the group with no known previous history (24 of 35). Nine of 15 with a known history of substance abuse died from the results of their alcoholism or drug addiction, and the death was coded as mental disorder with dependence syndrome, but this group was also represented by cardiovascular diseases and in ICD-10 Chapter XX (deaths from external causes). Altogether six of 11 deaths from external causes were regarded as likely suicides.
|
Table 3 Underlying cause of death after medical autopsies performed at Akershus University Hospital of deaths outside hospital in the period 2007 – 2011.
|
|
ICD-10 chapter
|
Number
|
|
II Neoplasms
|
4
|
|
IV Endocrine etc.
|
3
|
|
V Mental disorder
|
10
|
|
VI Nervous system
|
6
|
|
IX Cardiovascular diseases
|
40
|
|
X Respiratory system
|
7
|
|
XI Digestive system
|
3
|
|
XVII Congenital malformation
|
2
|
|
XVIII Uncertain cause
|
3
|
|
XX External cause
|
11
|
|
Total
|
89
|
A forensic toxicological examination was undertaken in 43 of the 89 autopsies, and the results were regarded as useful for the clarification of the underlying cause of death in 34 cases. This applied to negative findings in particular. Not unexpectedly, such special investigations were requested most frequently in cases of known substance or alcohol abuse (13 of 15 deaths) or mental disorder (five of six deaths), more rarely in cases of deaths where a treatment of somatic diseases had recently been initiated (two of 14). In those nine cases where a forensic toxicological examination was undertaken, but the results were regarded as having no value for the final decision, the cause of death was later determined with the aid of subsequent microscopy of organs and/or microbiological analysis.
Discussion
As a rule, studies of deaths that have occurred outside hospital tend to focus on forensic issues or sudden unexpected death. The author has found no studies of the frequency of medical autopsies of deaths outside hospital, either in Norway or internationally. A comparison with the autopsy material for the entire country from 2005, which primarily refers to deaths in hospital, shows that those who died outside hospital and were autopsied at Akershus University Hospital were significantly younger (12 and 11 years of difference in median age for men and women respectively), the proportion of men was higher (67 % compared to 56 % nationwide), neoplasms were more rare (4 % compared to 25 % nationwide) and that deaths from external causes were more frequent (12 % compared to 3 % nationwide) (11). The proportion of deaths from cardiovascular diseases was identical, which is due to a high proportion of deaths from this cause in the group with no known previous history and observed acute death.
When the current Act relating to hospital autopsies was written in the 1970s, most deaths occurred in hospital, and the autopsy frequency in institutions with a pathology department occasionally reached 80 % (3, 12). Today, most deaths occur in nursing and health institutions (4). These institutions only rarely have a tradition for requesting an autopsy. Only ten of the deaths in our material originated in nursing or health institutions.
The proportion of deaths occurring outside hospital or other health institutions has remained relatively stable, and account for approximately 20 % of the total (4). A large proportion of these deaths are unnatural according to the legislative definition. With the exception of those that obviously fall under this category, such as homicides, suicides and substance abuse, cases of unexpected death, deaths from unknown causes or deaths after recent contact with the health services may also be unnatural (Box 1). Many of these were therefore previously submitted to a forensic examination (13). In the early 1990s, the responsibility for the costs of forensic post mortems was transferred from the Ministry of Justice to the police districts – and the proportion of forensic post mortems fell sharply (8).
The statistics for deaths that are currently investigated forensically permit no detailed analysis on the basis of gender, age or diagnosis, and there are large geographic variations in practices related to requisitioning (13). Nevertheless, we may assume that the need for a better analysis of the group of deaths that occur outside institutions, which no longer are investigated forensically, may be one explanation for why the number of medical autopsies of these cases has increased, in the country as a whole as well as in Akershus University Hospital. Even though the autopsy records reviewed do not systematically register whether the death was reported as unnatural or not, the circumstances and the clinical information indicate that at least half of the autopsies must have related to deaths that were regarded as unnatural prior to this procedure.
The distribution of medical autopsies of deaths outside hospital between the first and second half of the year, shown in Figure 2, is striking. Since many of these cases fall within the definition of unnatural death, it is not unreasonable to speculate that the reason why the number of autopsies increases towards the end of the budget year may be found in restrictive practices with regard to requests for forensic post mortems in the police districts.
A forensic toxicological examination was deemed to be useful in 34 of the 89 cases of death (38 %). In four cases, such examinations revealed that the cause of death was intoxication with pharmaceutical drugs, in three cases probably ingested with suicidal intent. In this context, it is noteworthy that public suicide statistics fluctuate in line with the frequency of post mortems (14, 15). The cost of a forensic toxicology examination in the Norwegian Institute of Public Health exceeds the reimbursement rate for a medical autopsy of a death that has occurred outside hospital (7). The discrepancy between the cost and the reimbursement rate may induce the pathologists to be more restrictive in their requests for forensic toxicological examinations. The number of such examinations for the autopsies performed is therefore most likely the minimum deemed to be necessary.
The Cause of Death Registry has previously estimated that in 11.7 % of all medical autopsies performed in 2009, death had occurred outside a health institution, but it is uncertain whether deaths in ambulances are included in this estimate (8). For the same reason, the figures from the Cause of Death Registry that are used in this study are not comparable to the development observed in Akershus University Hospital. The fact that figures from the registry show an increase of 45 % from 2007 to 2010, while the number of medical autopsies has remained stable, is nevertheless an indication that the number of autopsies for deaths that have occurred outside hospital is increasing nationwide as well.
Conclusion
The number of medical autopsies of deaths outside hospital increased in the period 2007 – 2011, both in the Department of Pathology of Akershus University Hospital and nationwide. A large proportion of these deaths were initially regarded as unnatural, but were often resolved as being from natural causes during the autopsy. Medical autopsies of deaths outside hospital differed from the general nationwide autopsy material, in that the deceased tended to be younger, the proportion of men was larger, there was more often an absence of a previous medical history and more frequently the deaths had occurred from external causes. A forensic toxicological examination was also useful in the assessment of the cause of death in such autopsies.
