Pregnancy and lactation-associated osteoporosis is a rare condition. We describe a young patient who sustained multiple vertebral fractures after lifting a light object.
A primiparous woman in her late twenties with severe back pain two weeks post-partum was diagnosed with multiple vertebral fractures on magnetic resonance imaging and low lumbar spine bone mineral density (BMD) for her age. She was successfully treated with daily teriparatide subcutaneously and calcium and vitamin D supplementation for 2 years, and thereafter zoledronic acid intravenously. After three years’ follow-up, lumbar spine BMD had increased by 36 %. Pregnancy and breastfeeding are associated with bone loss because calcium is transferred from the mother to build the fetal and infant skeleton. Osteoporosis during pregnancy or breastfeeding is a rare condition characterised by high bone turnover, bone loss and fragility fracture(s), most commonly vertebral fractures with severe back pain. Causes of the condition are unknown; however, those who are affected often have an eating disorder, low intake of calcium or vitamin D, or a family history of osteoporosis. Early and correct diagnosis and treatment are essential.
A primiparous woman in her late twenties developed acute back pain two weeks post-partum after lifting a light object. The pain was localised between the shoulder blades and in the lower thoracic spine. She was otherwise healthy, a non-smoker, had a normal diet and had exercised three times a week prior to the pregnancy. She had become pregnant after in vitro fertilisation. At her first antenatal appointment, she was 168 cm and 55 kg; at the time of the birth she weighed 69 kg. The pregnancy had progressed normally, with the exception of pelvic pain that was treated by a physiotherapist and chiropractor. The birth was uncomplicated, and the infant was exclusively breastfed.
When the back pain had not resolved after three months, the patient was referred to the orthopaedic outpatient clinic, where examination revealed pain upon palpation and movement of the thoracic spine. Magnetic resonance imaging (MRI) showed fractures and bone marrow oedema in the superior endplate of vertebral body T7, the inferior endplate of T9 (Figure 1), and in the superior and inferior endplates of L1 and L3 (Figure 2).

Figure 1 Sagittal T1-weighted magnetic resonance imaging of the thoracic spine showing fractures and bone marrow oedema in the superior endplate of vertebral body T7 and in the inferior endplate of T9 and L1
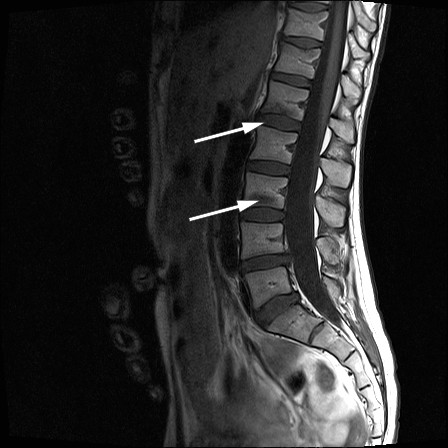
Figure 2 Sagittal T1-weighted magnetic resonance imaging of the lumbar spine showing fractures and bone marrow oedema in the inferior endplates of L1 and L3.
The patient was referred to the department of rheumatology to be assessed for possible osteoporosis. She had no family history of osteoporosis and no previous fractures. During her pregnancy, she had taken nutritional supplements for pregnant women that included calcium and vitamin D. She was advised to stop breastfeeding to avoid further bone loss (1, 2). Blood tests showed a normal sedimentation reaction and normal values for C-reactive protein, creatinine, vitamin D, calcium, parathyroid hormone, phosphate, magnesium, sodium, potassium, thyroid-stimulating hormone, thyroxine, alkaline phosphatase, alanine aminotransferase, serum transglutaminase antibody and serum protein electrophoresis.
Bone mineral density (BMD) at the lumbar spine as measured by dual energy X-ray absorptiometry was lower than expected for the patient’s age (Figure 3, Figure 4). The very low BMD and multiple vertebral fractures were interpreted as pregnancy and lactation-associated osteoporosis.
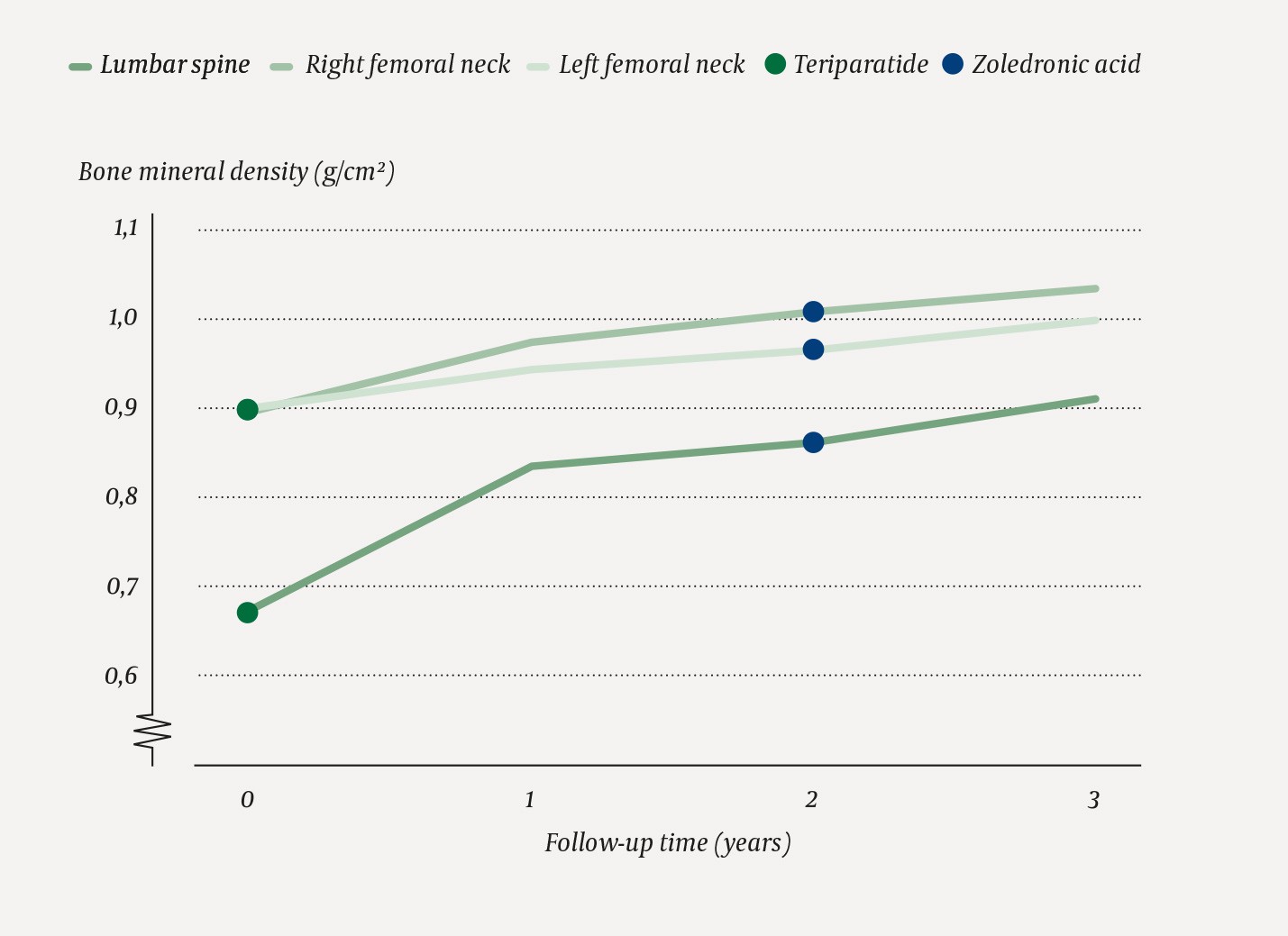
Figure 3 Annual bone mineral density (g/cm2) in the lumbar spine and in the right and left femoral neck as measured by dual energy X-ray absorptiometry during treatment.
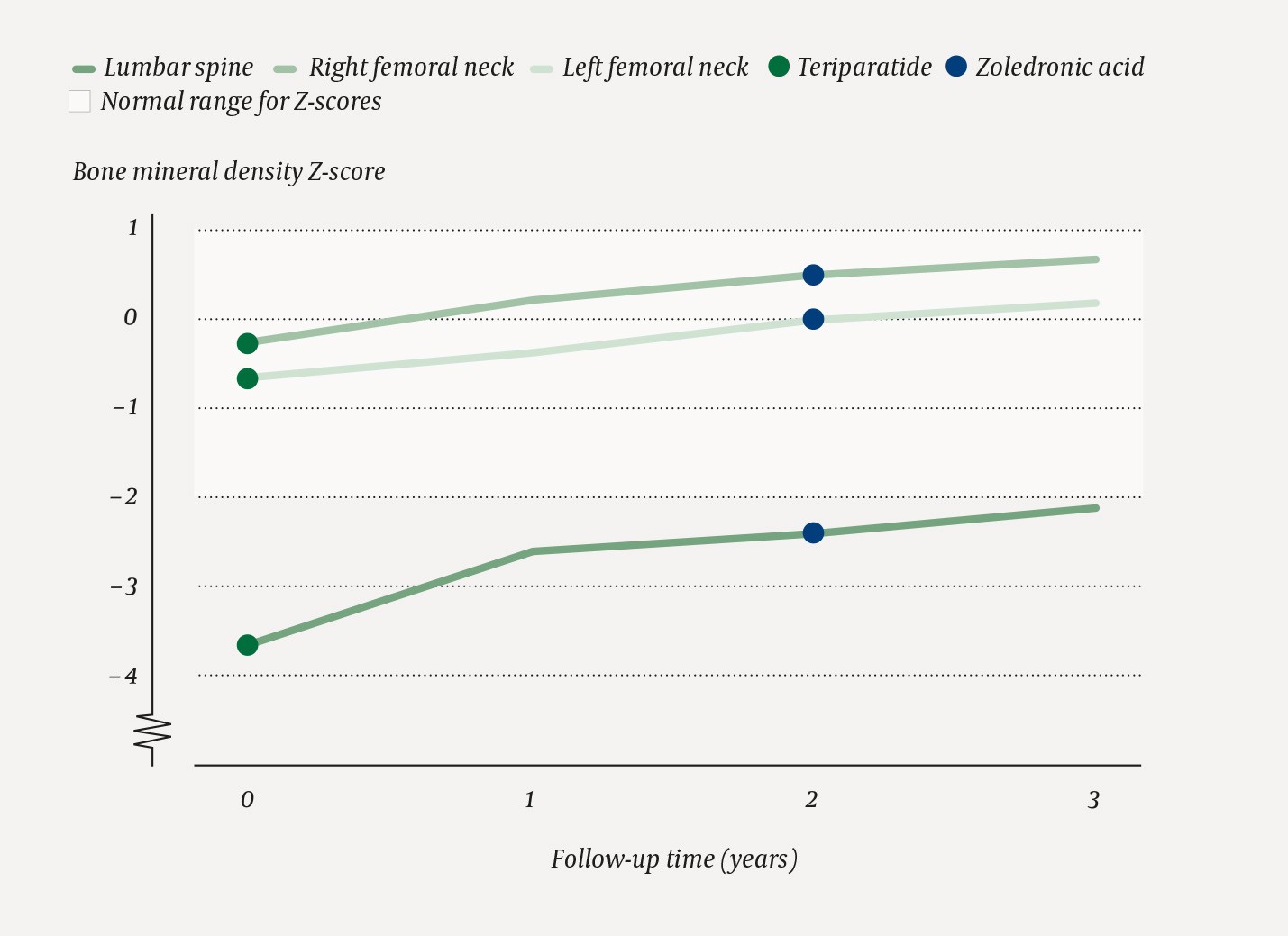
Figure 4 Annual Z-score (standard deviation from the average value for age) of bone mineral density at the lumbar spine and atthe right and left femoral neck. Lighter area of the graph shows expected Z-scores for age.
The patient was started on 20 µg teriparatide subcutaneously and 1 000 mg calcium and 800 IU vitamin D per os daily. She was prescribed sick leave and the child’s father took over the parental leave. She was followed up by a doctor, osteoporosis nurse, physiotherapist and occupational therapist in the osteoporosis unit. Treatment with teriparatide was continued for two years, and was followed by a dose of 5 mg zoledronic acid intravenously. BMD was measured annually. After three years, it had increased by 36.2 % at the lumbar spine, 14.5 % at the right femoral neck and 11.7 % at the left femoral neck compared with baseline values (Figure 3). BMD increased at all sites measured; after three years, it was just below the expected level for the patient’s age at the lumbar spine (Figure 4). Zoledronic acid is usually administered once yearly, but the subsequent dose was postponed because the patient was planning a new pregnancy and treatment with bisphosphonates during pregnancy is contraindicated.
Discussion
Pregnancy and breastfeeding result in transient bone loss because calcium is transferred from the mother to build the fetal and infant skeleton (1, 3). Pregnancy and lactation-associated osteoporosis is characterised by high bone turnover, which is first expressed through the loss of trabecular bone tissue, where the bone surface area to volume ratio is largest (3). Compression fractures in the lower thoracic or lumbar spine are most common. The cause of the condition is unknown, but those affected often have a history of eating disorder, a low intake of calcium or vitamin D, or a genetic predisposition to osteoporosis (4).
Back pain resulting from vertebral fractures may be pronounced with a transient or chronic course. Early diagnosis and treatment are important to prevent further fractures with chronic pain, as well as to optimise bone structure (5).
Our patient had significant back pain and had been unable to lift her child for three months prior to the condition being diagnosed. She was advised to stop breastfeeding. Exclusive breastfeeding is usually recommended for up to six months if the condition does not require immediate drug treatment. Bone resorption inhibitors in the form of bisphosphonate tablets are often first-line treatment. These are inexpensive and easy to administer. However, the effectiveness of this treatment has not been documented in premenopausal women, and should be used with caution in women who are planning a pregnancy (6).
We treated the patient with osteoanabolic therapy in the form of teriparatide for 24 months because of her many vertebral fractures, significant pain and very low bone mineral density at lumbar spine (3.7 standard deviations below the level expected for her age). Individual case reports have described the effectiveness of teriparatide in this condition (7). Zoledronic acid was given shortly after the last dose of teriparatide in order to consolidate the anabolic effect.
Pregnancy and lactation-associated osteoporosis occurs more frequently in first pregnancies than in later pregnancies (7). The aim of treatment was to bring the bone mineral density up to a level where the patient could have another pregnancy and subsequently breastfeed with the lowest possible risk of new vertebral fractures. Interdisciplinary follow-up was important for ensuring rapid treatment and resumption of normal activity levels.
