Pocket-sized ultrasound devices have been on the market for about ten years. The price of a pocket ultrasound device is relatively low compared to that of a conventional ultrasound scanner, and pocket devices are highly portable and require little additional training to use. Their functionality is somewhat reduced compared to that of conventional scanners, with a limited range of probes, lower penetration, lower resolution, a smaller screen and an inability to measure velocity. Nevertheless, pocket ultrasound devices have proven to be a useful tool in several clinical settings. For echocardiography (1, 2) and intra-abdominal examinations (3), pocket devices have been shown to be useful and cost-effective for screening and simpler diagnostics (4).
Within the field of vascular surgery, pocket ultrasound devices have proven to be useful in screening for abdominal aortic aneurysms and for measuring aneurysm diameter (5, 6), as well as for diagnosing complications after catheterisation of the femoral artery during coronary angiography (7).
The aim of our study was to investigate whether vascular surgeons could benefit from using a pocket ultrasound device in everyday clinical practice.
Material and method
The Department of Vascular Surgery at St. Olavs Hospital, Trondheim University Hospital has ten beds. The surgical interventions performed include open and endovascular aortic surgery, peripheral vascular surgery, and open and endovenous ablation of varicose veins. In 2017, around 250 open arterial procedures were performed. Conventional ultrasound scanners are available in outpatient clinics, Acute Admissions and operating theatres. Use of ultrasound scanners on wards, during surgery or while on call is an integral part of clinical practice and is not recorded.
A prospective study was conducted in the period from May 2017 to February 2018. All doctors (eleven in total) who performed ultrasound examinations in the department participated in the study. Two ‘Vscan Dual Probe’ pocket-sized ultrasound devices (GE Vingmed Ultrasound, Horten, Norway) were placed on the ward so that they were easily accessible. The Vscan device has two transducers in a single probe. The probe for superficial use has a dedicated vascular program, with frequencies from 3.4 to 8.0 MHz. There is no capacity to measure velocity, but there is a colour Doppler function. A one-hour introductory course was held prior to study start-up.
Participants were free to choose between a conventional ultrasound scanner and a pocket ultrasound device for ultrasound examinations. After each use of the pocket device, participants completed a registration form with information including: the reason the examination was required (ten predefined indications), whether the clinical question was answered (yes or no), a subjective rating of image quality (good, moderate, or poor), any supplementary diagnostic imaging required (ultrasound, CT, or other) and the examiner’s experience with ultrasound (< 1 year, 1–3 years, 3–5 years or > 5 years) (see registration form in Appendix 1). From a review of medical records, we were able to estimate the number of operations that required preoperative ultrasound marking (Table 1).
Table 1
Number of ultrasound examinations performed with the Vscan pocket ultrasound device during the study period, and the extent to which use of the Vscan answered the clinical question, for eight of a possible ten indications (no examinations were performed for two predefined indications). For certain indications, ultrasound examination is always performed and thus the total number of ultrasound examinations was known.
|
Indication
|
Total number of ultrasound examinations in study period
|
Performed with Vscan device
|
Clinical questions answered with Vscan device
|
|
Vein marking prior to varicose vein surgery
|
60
|
15
|
14 (93 %)
|
|
Vein mapping prior to femoropopliteal bypass surgery
|
13
|
10
|
10 (100 %)
|
|
Vein mapping prior to construction of an arteriovenous fistula
|
27
|
10
|
8 (80 %)
|
|
Preoperative assessment of carotid artery (location of bifurcation, open internal carotid artery)
|
Not available1
|
8
|
5 (63 %)
|
|
Evaluation of pseudoaneurysm - femoral artery
|
Not available1
|
6
|
5 (83 %)
|
|
Evaluation of pseudoaneurysm - radial artery
|
Not available1
|
2
|
0 (0 %)
|
|
Checking of femoropopliteal bypass
|
Not available1
|
6
|
5 (83 %)
|
|
Other
|
|
3
|
4 (100 %)
|
|
Total
|
|
60
|
51 (85 %)
|
To determine whether conventional ultrasound scanners or pocket ultrasound devices were preferred, participants were asked to complete a questionnaire at the end of the study period (see Appendix 2). Participants considered which type of apparatus they preferred for particular indications (‘Always a conventional ultrasound scanner’, ‘Always Vscan’ or ‘It depends’), as well as the factors that determined their choice of ultrasound apparatus (nine statements rated on a scale from 1 (‘Strongly disagree’) to 5 (‘Strongly agree’).
The Regional Committee for Medical and Health Research Ethics (REC) considered the study to be a quality assurance study and thus exempt from the requirement for approval.
Results
A total of 60 registration forms were completed after use of a pocket-sized ultrasound device. Pocket devices were not used for all predefined indications. All eleven doctors recorded use of a pocket device (2–18 examinations per doctor). Four doctors had 1–3 years of experience with ultrasound, and seven doctors had more than 5 years of experience.
Pocket ultrasound devices answered the clinical question in 51 (85 %) of the 60 examinations for which they were used. Pocket devices were used for venous applications in 35 of 60 cases – for preoperative marking of veins prior to varicose vein ablation, femoropopliteal bypass surgery or the construction of an arteriovenous fistula. Detailed results for each indication are summarised in Table 1. Forty-three of 60 examinations with a pocket ultrasound device were performed preoperatively, mainly in situations where vein marking was required. The pocket device answered the clinical question in 32 (91 %) of 35 such cases. In cases of vein mapping prior to bypass surgery, pocket ultrasound devices were used in 10 (77 %) of 13 cases, and the clinical question was answered in all 10 cases without the need for supplementary diagnostic testing.
The image quality was rated as good in 32 (53 %) examinations performed with a pocket ultrasound device, moderate in 21 (35 %) and poor in 7 (12 %). Within these categories, the clinical question was answered in 30 (94 %), 19 (90 %) and 2 (29 %) cases, respectively. Supplementary diagnostic testing was performed in 12 cases, but in only 8 of these was the clinical question not answered.
The questionnaire completed at the end of the study period revealed that the main reason for not using a pocket ultrasound device was an expectation that the image quality would be inadequate (Figure 1, median 5, range 3–5). In those cases where a pocket device was chosen, accessibility was especially highly valued (median 5, range 1–5). The seven doctors with more than five years of ultrasound experience preferred conventional scanners in 60 % of cases, whereas the corresponding figure for those with less than five years of experience was 29 %.
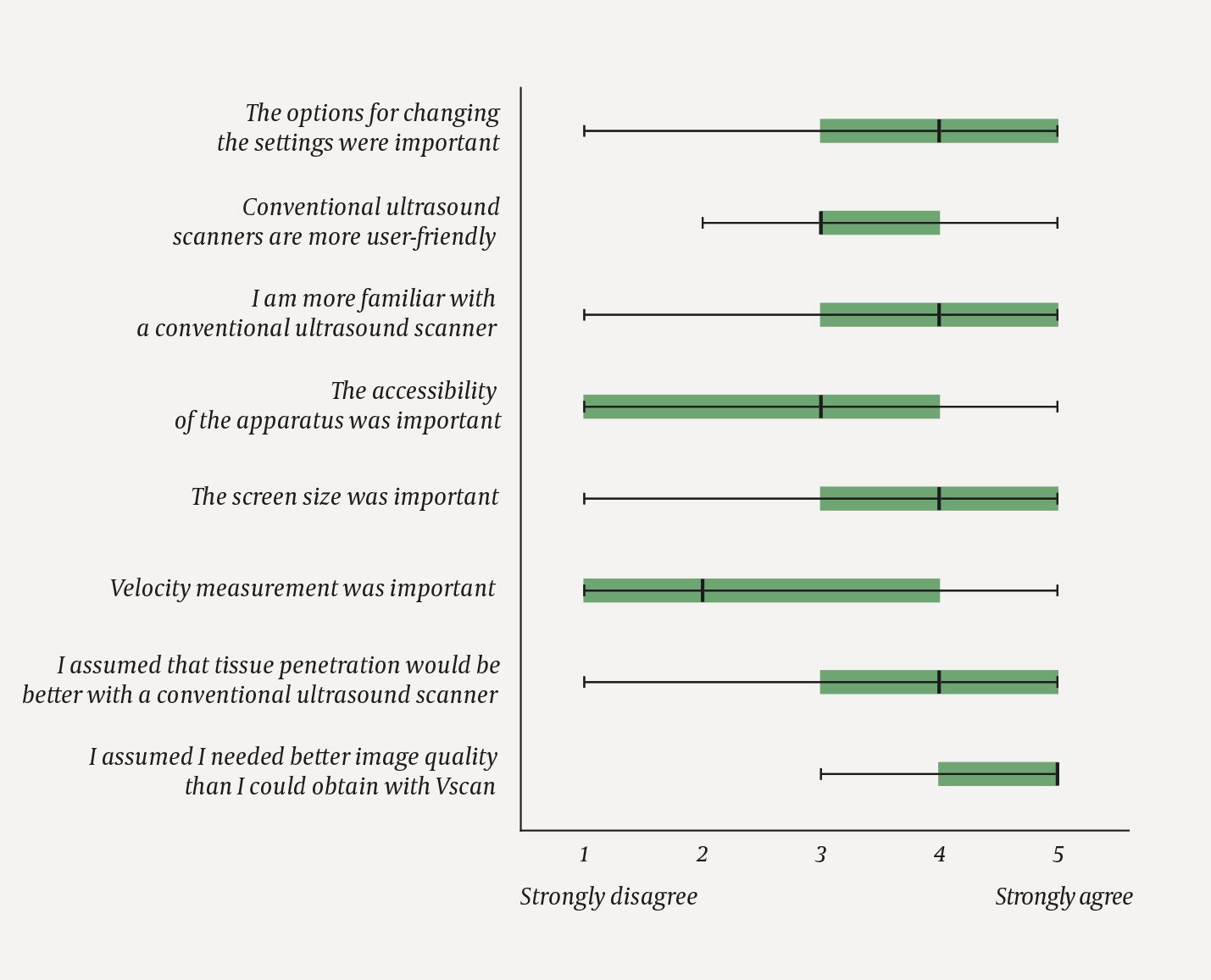
Figure 1 Box plots showing participants’ responses to the following question: “In a situation in which you thought Vscan was not good enough: on a scale of 1 (strongly disagree) to 5 (strongly agree), rate the extent to which the following statements apply to your choice”. The question was asked for each indication, and the box plots show the responses for all indications combined. The statement “Colour Doppler was important” has not been included, as both machines used colour Doppler. Each box plot shows the median, interquartile range, and range.
Discussion
This is a descriptive study of the use of a pocket ultrasound device by vascular surgeons, and not a direct comparison of conventional scanners and pocket devices. The possibility of selection bias, in which pocket devices were primarily used for more straightforward examinations, cannot be ruled out. Image quality was good or moderate in 53 of 60 examinations in which a pocket device was chosen as the initial imaging modality, and the clinical question was answered in 51 of 60 cases.
The pocket ultrasound device was used less than expected during the registration period. The most experienced doctors were less likely to use it, owing to a desire for higher image quality.
The availability of conventional ultrasound scanners is good in our hospital, which may help explain the relatively low number of pocket ultrasound examinations during the study period. An inability to measure velocity, which is important for assessing arterial blood flow, also means that the pocket device in question cannot replace a conventional scanner for all indications.
However, for simpler examinations in the context of vascular surgery, especially with respect to the venous system, a pocket ultrasound device can be a useful adjunct to conventional ultrasound scanners.
