The strategy to rein in the COVID-19 pandemic has been based on infection control and restrictions on the daily life of the population (1). Hand washing and social distancing (2) are especially important, but we know little about actual compliance with the infection control rules.
The academic literature is sparse, but a study conducted in the UK in March 2020 showed that 93 % had taken at least one precaution to protect themselves against COVID-19 (3). Most people washed their hands more frequently than before (83 %), and around one-half practised social distancing. A study from Hong Kong in January showed that 96 % reported more frequent hand washing, while 30–70 % engaged in various forms of social distancing. Compliance was lowest in the youngest age groups, and higher among women than among men (4). An American study that has not been peer reviewed and is based on a convenience sample of adolescents from March 2020 showed that 30 % had no contact with persons outside their own household, while 88 % washed their hands frequently (5). Another study from March 2020, also not peer reviewed, showed that a large proportion of Norwegian adults had changed their behaviour to limit the spread of infection, and that as many as 92 % practised frequent hand washing (6).
Economically disadvantaged groups and ethnic minorities appear to be especially hard-hit by the COVID-19 pandemic. In the United States, this applies to African-Americans in particular (7), and one reason may be insufficient compliance with infection control rules (8). Data from Oslo show that districts in the wealthy parts of western Oslo were strongly affected at the early stage of the pandemic, but that infection rates gradually increased more in the outer eastern suburbs, where the population has low incomes, little education and includes many immigrants. In mid-May 2020, the Stovner, Alna and Grorud districts had the highest number of infections per inhabitant, and immigrants were overrepresented among the newly reported COVID-19 cases (9, 10). Many factors can conceivably help explain the infection rate in the eastern part of the city, such as residential crowding or socioeconomic factors. However, local variations in compliance with infection control rules and variations by wider sociodemographic characteristics may also play a role. We know little about such variations.
In general, socioeconomic status and concurrent inequalities in health-related lifestyle are strong predictors of morbidity (11). Women tend to comply with health-related advice more frequently than men (11), and Norwegian data indicate that women take more precautions against infection (6). Furthermore, the countries that are hardest affected by the COVID-19 pandemic appear to be characterised by little trust between people and in the authorities (12). It seems as though Norwegians trust the health authorities in their handling of the COVID-19 pandemic, but we know little about what this means for protective behaviour. On the whole, lower compliance with infection control is likely to be found among men and in groups with little education, weak socioeconomic resources and low levels of trust. Acceptance of the infection control rules might also be important (1).
We wanted to elucidate the extent to which adolescents in Oslo report to comply with the infection control rules during the COVID-19 pandemic. We investigated whether this varies by sociodemographic characteristics, acceptance of the infection control rules and confidence that the COVID-19 pandemic is being well managed by the authorities and by people in general.
Material and method
Procedure and participants
The study Oslo-ungdom i koronatiden [Adolescents in Oslo in the time of the coronavirus] was undertaken from 23 April to 8 May 2020. At the start of the study, the schools had been closed for six weeks and had switched to home teaching. Strong restrictions had been placed on social interaction. The infection control rules were reported in the daily newscasts. All state schools in Oslo were asked to participate by setting aside 30 minutes of a home teaching session, and 37 % of the students participated (N = 12 686). The response rate was higher in lower secondary schools (46 %, n = 8 116) than at the upper secondary level (27 %, n = 4 552; 18 students did not report their grade). The proportion of missing data varied from 0 % (n = 13) for sex to 14 % (n = 1 824) for trust in the handling of the COVID-19 pandemic by the prime minister and the government (the question was asked towards the end of the questionnaire).
We compared sociodemographic characteristics in our sample with public statistics on Oslo adolescents in the same age group, which we retrieved from Statistics Norway for sex and immigrant background (13) and from the City of Oslo for district (14). The proportion of girls was higher in the study (57 % vs. 50 %), there were fewer from immigrant backgrounds (31 % vs. 37 %) and fewer who were resident in the outer and inner eastern suburbs of Oslo (45 % vs. 49 %).
The study was conducted by the NOVA research centre at Oslo Metropolitan University in collaboration with the City of Oslo educational authorities. The students were provided with written information stating the study’s objectives and that participation was voluntary. Parents were informed through the Oslo schools’ digital information system (‘Skolemelding’). The study was anonymous and not subject to submission before the Regional Committee of Medical and Health Research Ethics. A draft questionnaire was tested among students and assessed by a reference group that included teachers.
Variables
Compliance with infection control rules. No validated instruments are available for measuring protective behaviour during pandemics (15). One exception is an instrument from a non-peer reviewed study which is not adapted to adolescents or to Norwegian conditions (15). We therefore developed our own instrument based on the infection control recommendations from the Norwegian Institute of Public Health (2). We asked: ‘To what extent have you complied with the advice from the health authorities to reduce infections?’ We described four rules: ‘Washed your hands with soap or hand sanitiser after having been to public places’, ‘Avoided shaking hands with or hugging other people’, ‘Kept a good distance (1–2 metres) from people other than those you are living with’ and ‘Avoided groups of more than five persons’. The response alternatives were 1 (not at all), 2 (to a small extent), 3 (to a fairly large extent), 4 (to a large extent) and 5 (always). Answers were combined into an average score, and scores of 4 or higher were categorised as a high degree of compliance with the rules.
Sociodemographic variables. We asked about participants’ sex and grade. Place of residence was classified into four regions of Oslo: western Oslo (Vestre Aker, Nordre Aker, Ullern, Frogner and St. Hanshaugen districts), inner eastern Oslo (Grünerløkka, Gamle Oslo and Sagene districts), outer eastern Oslo (Søndre Nordstrand, Bjerke, Stovner, Alna and Grorud districts) and Østensjø/Nordstrand (Østensjø and Nordstrand districts). The socioeconomic status of parents was measured based on the number of parents with higher education, the number of books in the home and the average score on the Family Affluence Scale II (number of cars and computers in the family, holiday trips and separate bedrooms) (16). An average score was constructed (16) and used to divide the sample into three equally sized parts: adolescents with low, medium and high socioeconomic status.
Immigrant background was defined as having two foreign-born parents. We asked for grades in English, Norwegian and mathematics and divided them into low (1.0–3.9), medium (4.0–4.9) and high (5.0–6.0) average grades.
Trust in the handling of the COVID-19 pandemic. We started by asking: ‘To what extent do you trust that those who are in charge in Norway are making a good job of tackling the coronavirus epidemic?’, followed by ‘The Prime Minister and the government’ and ‘the health authorities’. We also asked: ‘Do you trust that people will abide by the rules that have been introduced?’ Response categories for all questions were ‘not at all’, ‘to a small extent’, to a fairly large extent’ and ‘to a very large extent’. We dichotomised the three variables into those who had a fairly or very large level of trust, and contrasted them with all the others.
Acceptance of the infection control rules. We asked: ‘What do you think of all the rules that have been introduced to prevent the coronavirus from spreading (for example school closures, keeping two metres of distance, a maximum of five in each group)?’, with these response alternatives: ‘The rules are much too strict’, ‘The rules are as strict as they need to be’ and ‘The rules should be even stricter’.
Data processing and analyses
We used simple logistic regression analyses with a categorisation based on the aggregate measure of compliance with infection control rules as an outcome variable to investigate unadjusted associations with sociodemographic characteristics, trust and acceptance of the infection control rules. We subsequently used multiple regression analyses. In an initial model we included all sociodemographic characteristics simultaneously to investigate whether the association between such characteristics and the measure of compliance with infection control rules remained stable when adjusting for all other sociodemographic factors. In a final model we also included trust and acceptance of the infection control rules as predictors to investigate whether the associations remained stable when controlling for all predictor variables used in the study. In all the regression analyses we included only respondents who had answered all variables used in the analyses (N = 10 382).
Results
Figure 1 shows that 9 915 adolescents (84 %) reported to ‘always’ or ‘to a large extent’ wash their hands with soap or hand sanitiser after having been to public places. Many reported to avoid shaking hands or hugging (n = 8 730, 74 %) or being in large groups (n = 8 565, 73 %), while 5 859 adolescents (50 %) reported that they always or to a large extent maintained 1–2 metres distance from others. Based on the average score and the categorisation described above, 7 304 (62 %) of the 11 806 adolescents who had responded to the questions about infection control reported to comply with the infection control rules to a large extent.
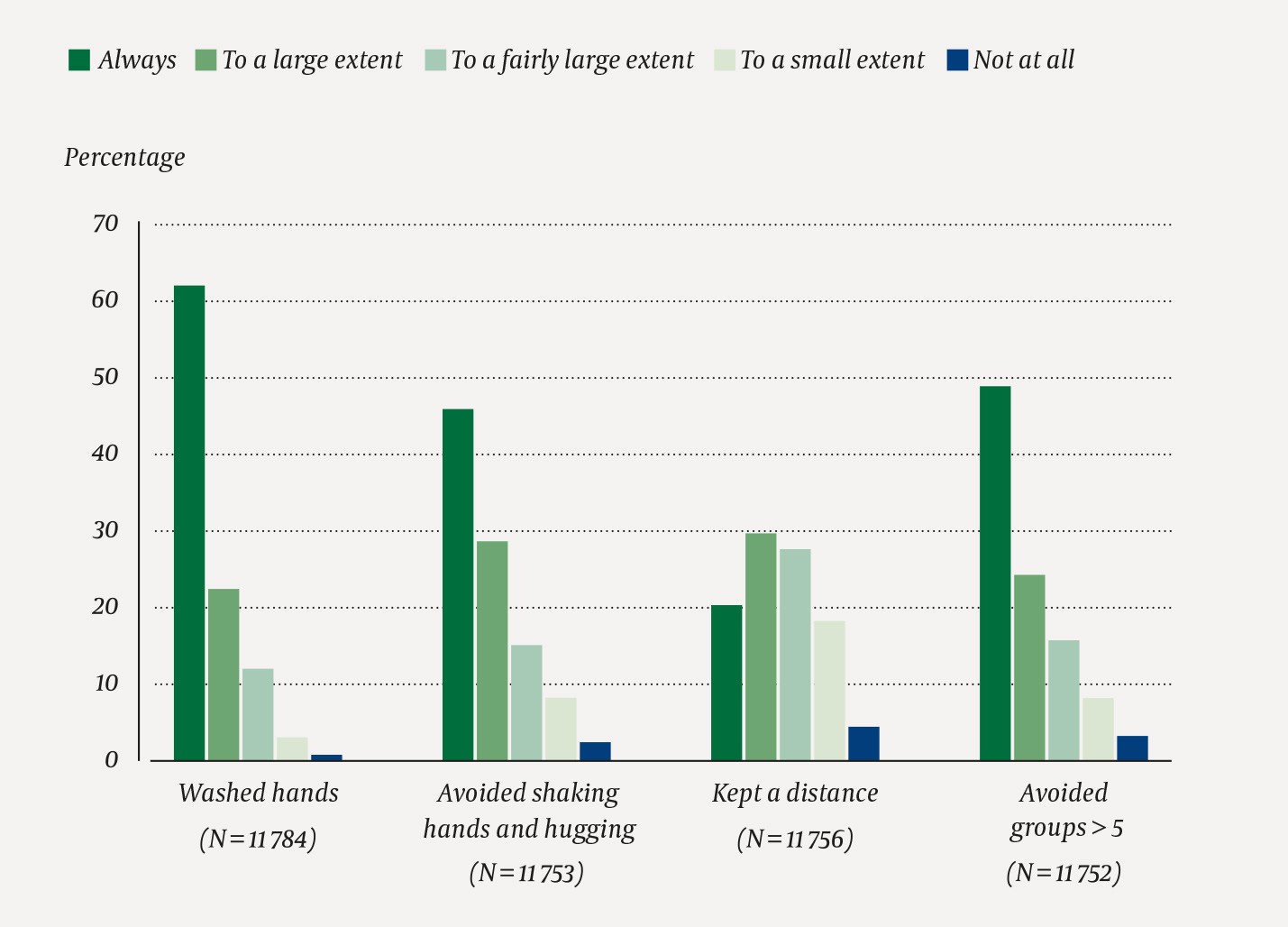
Figure 1 Proportion of respondents reporting to comply with different infection control rules during the COVID-19 pandemic. Adolescents in Oslo completed the questionnaire between 23 April and 8 May 2020.
Figure 2 shows that 9 962 adolescents (92 %) had a fairly or very large trust in the health authorities’ handling of the pandemic. The corresponding figure for the prime minister and the government was n = 8 742 (80 %). The adolescents were less confident that people in general would comply with the infection control rules (n = 5 255, 48 %). 8 408 (77 %) were of the opinion that the rules were as strict as they needed to be, 986 (9 %) felt that the rules were too strict, and 1 547 (14 %) believed that the rules should be even stricter.

Figure 2 Proportion of respondents who reported to have trust in the authorities’ handling of the COVID-19 pandemic and that people in general complied with the infection control rules. Adolescents in Oslo completed the questionnaire between 23 April and 8 May 2020.
We investigated whether reported compliance was associated with sociodemographic factors (Table 1). A larger proportion of the girls (67 %) than boys (55 %) complied with the infection control rules to a large extent. Students in the two last years of upper secondary school and adolescents from immigrant backgrounds most often reported to comply with the rules. The same applied to adolescents living in the outer eastern suburbs of Oslo. Reported infection control behaviour varied little with the parents’ socioeconomic status. However, students with higher average grades reported to comply with the rules more often when compared to those with lower average grades.
Table 1
Proportion of respondents reporting that they always or to a large extent complied with the infection control rules during the COVID-19 pandemic, by sociodemographic characteristics. Adolescents in Oslo completed the questionnaire between 23 April and 8 May 2020
|
|
Complied with the infection control rules to a large extent or always, number (%)
|
|
Sex (N = 11 715)
|
|
|
|
Boy
|
2 727 (55)
|
|
|
Girl
|
4 532 (67)
|
|
School year (N = 11 792)
|
|
|
|
8th grade
|
1 660 (61)
|
|
|
9th grade
|
1 319 (60)
|
|
|
10th grade
|
1 568 (60)
|
|
|
Upper secondary, 1st year
|
1 078 (60)
|
|
|
Upper secondary, 2nd year
|
852 (67)
|
|
|
Upper secondary, 3rd year
|
817 (72)
|
|
Immigrant background (N = 11 741)
|
|
|
|
At least one Norwegian-born parent
|
4 936 (60)
|
|
|
Two foreign-born parents
|
2 323 (67)
|
|
Place of residence in Oslo (N = 11 664)
|
|
|
|
Western Oslo
|
2 272 (60)
|
|
|
Østensjø and Nordstrand
|
1 646 (60)
|
|
|
Inner east
|
762 (59)
|
|
|
Outer east
|
2 530 (66)
|
|
Socioeconomic status (N = 10 382)
|
|
|
|
Low
|
2 379 (63)
|
|
|
Medium
|
2 283 (60)
|
|
|
High
|
2 605 (63)
|
|
Average grades (N = 10 581)
|
|
|
|
Low grades (1–3.9)
|
1 812 (58)
|
|
|
Medium grades (4–4.9)
|
3 065 (62)
|
|
|
High grades (5–6)
|
1 736 (69)
|
High trust was related to reported compliance with the rules, with approximately equal odds ratios for all three indicators of trust (see Tables 2 and 3). The proportion that reported to comply with the rules to a large extent was lower among those who felt that the rules were too strict (40 %), when compared to those who felt that they were appropriately strict (64 %) and those who claimed that the rules should be even stricter (71 %) (Table 2).
Table 2
Proportion of respondents reporting to comply with the infection control rules to a large extent or always during the COVID-19 pandemic by trust in the government, the health authorities and people in general, and acceptance of the infection control rules. Adolescents in Oslo completed the questionnaire between 23 April and 8 May 2020.
|
|
|
Complied with the infection control rules to a large extent or always, number (%)
|
|
Trust in the prime minister/government (N = 10 848)
|
|
|
|
Little or no trust
|
1 194 (57)
|
|
|
Fairly or very large trust
|
5 605 (64)
|
|
Trust in the health authorities (N = 10 843)
|
|
|
|
Little or no trust
|
490 (55)
|
|
|
Fairly or very large trust
|
6 312 (63)
|
|
Trust in people to comply with the infection control rules (N = 10 938)
|
|
|
|
Little or no trust
|
3 319 (58)
|
|
|
Fairly or very large trust
|
3 529 (67)
|
|
Acceptance of the infection control rules (N = 10 924)
|
|
|
|
Are exactly as strict as they need to be
|
5 361 (64)
|
|
|
Are too strict
|
395 (40)
|
|
|
Should be even stricter
|
1 095 (71)
|
Table 3
Associations between different explanatory variables and reporting of compliance with the infection control rules to a large extent or always among adolescents in Oslo during the COVID-19 pandemic. N = 10 382 adolescents who answered all the relevant questions in the questionnaire 23 April–8 May 2020 were included in simple (Model 1) and multiple regression analyses with sociodemographic factors (Model 2) and sociodemographic factors, trust and acceptance (Model 3) respectively as predictor variables. OR = odds ratio, CI = confidence interval.
|
|
|
Model 1
Unadjusted OR (95 % CI)
|
Model 2
Adjusted OR (95 % CI)
|
Model 3
Adjusted OR (95 % CI)
|
|
Sex (reference: boy)
|
|
|
|
|
|
Girl
|
1.60 (1.47–1.73)
|
1.53 (1.41–1.66)
|
1.47 (1.35–1.60)
|
|
School year (reference: 8th grade)
|
|
|
|
|
|
9th grade
|
1.01 (0.90–1.15)
|
1.00 (0.88–1.13)
|
0.96 (0.84–1.09)
|
|
|
10th grade
|
0.96 (0.86–1.08)
|
0.94 (0.84–1.06)
|
0.89 (0.79–1.01)
|
|
|
Upper secondary, 1st year
|
1.02 (0.89–1.16)
|
1.01 (0.89–1.16)
|
0.99 (0.86–1.13)
|
|
|
Upper secondary, 2nd year
|
1.34 (1.15–1.55)
|
1.29 (1.11–1.50)
|
1.25 (1.07–1.46)
|
|
|
Upper secondary, 3rd year
|
1.60 (1.36–1.87)
|
1.56 (1.33–1.84)
|
1.52 (1.29–1.79)
|
|
Immigrant background (reference: at least one Norwegian-born parent)
|
|
|
|
|
|
Two foreign-born parents
|
1.34 (1.23–1.47)
|
1.41 (1.26–1.57)
|
1.46 (1.31–1.64)
|
|
Place of residence in Oslo (reference: western Oslo)
|
|
|
|
|
|
Østensjø and Nordstrand
|
1.00 (0.90–1.12)
|
1.08 (0.97–1.20)
|
1.10 (0.98–1.23)
|
|
|
Inner east
|
0.99 (0.86–1.14)
|
1.02 (0.89–1.19)
|
1.05 (0.91–1.22)
|
|
|
Outer east
|
1.30 (1.18–1.44)
|
1.34 (1.19–1.50)
|
1.35 (1.20–1.51)
|
|
Socioeconomic status (reference: low status)
|
|
|
|
|
|
Medium
|
0.93 (0.84–1.02)
|
1.05 (0.94–1.17)
|
1.03 (0.92–1.15)
|
|
|
High
|
1.03 (0.94–1.14)
|
1.21 (1.08–1.36)
|
1.20 (1.06–1.35)
|
|
Average grades (reference: low grades)
|
|
|
|
|
|
Medium grades (4–4.9)
|
1.20 (1.10–1.32)
|
1.24 (1.13–1.37)
|
1.17 (1.06–1.29)
|
|
|
High grades (5–6)
|
1.60 (1.42–1.79)
|
1.61 (1.43–1.82)
|
1.54 (1.36–1.74)
|
|
Trust in the government (reference: low trust1)
|
|
|
|
|
|
High trust2
|
1.38 (1.25–1.52)
|
|
1.22 (1.08–1.38)
|
|
Trust in the health authorities (reference: low trust1)
|
|
|
|
|
|
High trust2
|
1.42 (1.24–1.63)
|
|
1.11 (0.94–1.32)
|
|
Trust in people (reference: low trust1)
|
|
|
|
|
|
High trust2
|
1.48 (1.36–1.60)
|
|
1.58 (1.45–1.72)
|
|
Rules (reference: are exactly as strict as they need be)
|
|
|
|
|
|
Are too strict
|
0.38 (0.33–0.44)
|
|
0.43 (0.37–0.49)
|
|
|
Should be even stricter
|
1.41 (1.25–1.59)
|
|
1.67 1.47–1.91)
|
The results of simple logistic regression analyses with unadjusted odds ratios are presented in Table 3, Model 1. The table shows that the results remained largely stable when we compare single with multiple analyses where all sociodemographic characteristics were included simultaneously (Table 3, Model 2), and the size of the odds ratios changed only little. In Model 3 we can see that the degree of trust in other people to comply with the rules was still related to reported compliance with the infection control measures, while the impact of trust in the government and the health authorities was somewhat reduced. The results also show that high socioeconomic status had a certain effect on compliance with the infection control rules after controlling for other socioeconomic characteristics (Models 2 and 3), while there was no such association in the unadjusted analyses (Model 1).
Discussion
We found that a clear majority of the adolescents in Oslo who responded to the survey reported to comply with the infection control rules to a large extent or always during the COVID-19 pandemic. However, it was only to the question of hand washing that a majority of the adolescents answered that they always complied with the rules. Adolescents from immigrant backgrounds and those living in the outer eastern suburbs reported higher compliance with the rules. Girls reported compliance with the rules more frequently than boys. A large majority trusted the authorities’ handling of the pandemic. On the other hand, fewer respondents trusted people in general to comply with the infection control rules. Nine out of ten believed that the rules were appropriately strict or could be even stricter. Trust in the authorities and in people in general and acceptance of the infection control rules were related to reported compliance.
The high level of trust in the health authorities indicates that they have communicated well with young people during the pandemic. Other Norwegian studies have shown that this also applies to adults (12). However, adolescents had less trust in people in general to comply with the infection control rules. This may have led to poorer compliance on their own part.
In line with previous research, girls reported to comply with the infection control rules to a higher extent than boys (4, 6). Reported compliance was lowest in the youngest age groups. This may be linked to the fact that the media and authorities have presented infection as less of a problem in young age groups. It is a new observation that adolescents from immigrant backgrounds in the outer eastern suburbs report higher compliance than others. The excess incidence of infection in these districts may be related to structural factors, such as residential crowding, the fact that many have jobs with high exposure to infection, and perhaps closer contact across generations. It is also conceivable that adolescents in the outer eastern suburbs were less careful about protective behaviour at the early stage of the pandemic, when the infection was less prevalent in these districts, and that they changed their behaviour when the spread of the infection intensified.
It is worth noting that those few (9 %) who felt that the infection control rules were too strict reported lower compliance. The causal relationship has not been identified, and it is conceivable that these respondents legitimise violations of the rules by toning down their importance. The findings nevertheless indicate that acceptance of restrictions is important for protective behaviour.
The strength of the study lies in being population-based, with a large sample. It was conducted at a time when strict restrictions were in force and when the pandemic defined the lives of these young people and their families. However, it also has some limitations. We used self-reporting, and the answers may have been tainted by the social desirability of compliance with the infection control rules (17). The estimate of compliance rates may thus be too high.
The advantage of our measure is that it was tested by both students and teachers and that we asked the adolescents to report how they complied with the infection control rules over a defined period of 6–8 weeks (from the time when the restrictions were introduced until the time when they participated in the study). This can be assumed to enhance reliability, compared to questions that measure longer time intervals retrospectively (17). We measured the degree of compliance with the rules, not the frequency of various types of behaviour. We thus do not know how often adolescents have been exposed to situations involving risk of infection. Such knowledge would have been useful for estimating the risk of actual infection. Furthermore, factors that are not included in the study, such as concerns of becoming infected (6), may have a bearing on infection control behaviour among adolescents.
The response rate is lower than in similar studies, such as the Ungdata and Young in Oslo surveys (16). Most likely, many teachers were unable to implement the survey at short notice. Moreover, the situation was less structured than when students respond to a questionnaire in the classroom. The data have a selection bias in relation to sociodemographic background variables. This attrition may be linked to compliance with the infection control rules, which could have an effect on the estimates.
The findings may also reflect the timing of the data collection. It was conducted 6–8 weeks after the strict restrictions were introduced. The news media and everyday life were dominated by the pandemic. Later studies may report other findings, because the authorities loosen the restrictions, because fatigue may set in among the population if the restrictions remain in place over a prolonged period, and because the focus on the heightened risk of infection in the eastern suburbs of Oslo may shift. Future studies will show whether the findings from Oslo can be generalised to other parts of Norway.
We conclude that a clear majority of the adolescents in Oslo who participated in the study reported to have complied with the infection control rules to a large extent. Most of them accepted that the rules were necessary, and they have high trust in the handling of the COVID-19 pandemic by the authorities. Some will be surprised that adolescents from immigrant backgrounds and those resident in the outer eastern suburbs of Oslo appear to comply with the rules to a larger extent than others. Later studies should elucidate such differences and their possible causes. More knowledge about this and other issues that we shed light on may contribute to even more effective measures to prevent the spread of infection.
