Studies show that some groups are more affected by the COVID-19 pandemic than others, both internationally and in Norway. A large study of socioeconomic factors in over one million cases in the United States found that a low level of education and an African-American background were strongly associated with infection, more severe symptoms and death as a result of COVID-19 (1).
Immigrants are overrepresented in infection statistics throughout Scandinavia (2). In Norway, 36 % of those with confirmed COVID-19 are immigrants born abroad to foreign parents, even though they only represent 15 % of the population (3). The most common explanations for the disproportionate rates include differences in somatic disease burden, living conditions and real opportunities for social distancing, e.g. because many work in service industries or live at close quarters and in cramped conditions. However, socioeconomic resources are also closely linked to immigrant status and ethnic background.
Oslo is a city with large disparities between districts and sub-populations. The tendency is for more cramped living conditions and a higher immigrant ratio in districts with a lower socioeconomic status (4). These also have significantly higher infection rates (5). The purpose of this study was to analyse the relationship between sociodemographic factors and infection rates in Oslo’s districts.
Material and method
On 3 December 2020, sociodemographic data were retrieved from Oslo City Government’s statistics database, whose data is sourced from Statistics Norway (4). Data on the cumulative number of registered cases of SARS-CoV-2 confirmed in a polymerase chain reaction (PCR) test as of 3 December 2020 were obtained from Oslo City Government’s Agency of Health (5).
In the analyses, we applied the same definitions as those used in the statistics database (4). Immigrants were defined as people born abroad to foreign parents (formerly called first-generation immigrants) or Norwegian-born with two parents born abroad (formerly called second-generation immigrants). Cramped living conditions were defined as households with more than one person per room or less than 20 square metres per person. Multi-family households were defined as households where the occupiers are made up of two or more families. Low level of education referred to 21–29-year-olds who had not completed upper secondary school. People aged 30–59 with no attachment to the labour market were defined as unemployed. Mean income was calculated on the basis of gross income per person over 16 years of age.
We created two composite variables. The formative variable socioeconomic status was created by converting the variables ‘education’, ‘income’ and ‘employment’ to the same scale (0 to 1) and taking an equally weighted average of these (6). Similarly, we converted the proportions in cramped living conditions and multi-family households to a variable that we called household density.
We first examined bivariate correlations for all variables in three of the statistics database’s sub-categories: population, living conditions and living conditions indicators, with registered cases of SARS-CoV-2 infection. In the further analysis, we selected variables that had a significant correlation with infection, with p <0.01 (alone or as part of a composite variable). We then calculated Pearson’s correlation coefficient between these variables and infection rates. Next, we performed a linear regression analysis using infection rates in the districts as a dependent variable and the two composite variables and immigrant ratio as independent variables, both separately and simultaneously in a multi-adjusted analysis. This analysis was weighted for the number of people in the districts.
The assumption of normal distribution was checked using a histogram of the residual plot. The analyses were performed in SPSS version 27.
The data are publicly available and are not personally identifiable. There was therefore no need to apply for permission to use the data.
Results
In total, there were approximately 688 000 inhabitants in the 15 districts of Oslo. The four districts in Groruddalen and Søndre Nordstrand had the most confirmed cases of infection: 2086–2623 cases per 100 000 inhabitants. These districts also had the highest immigrant ratios (44–59 %) and the highest proportions of people in cramped living conditions (15–17 %). The three western districts of Ullern, Nordre Aker and Vestre Aker, as well as the district of Nordstrand, had significantly lower infection rates: 893–1161 confirmed cases per 100 000 inhabitants, lower immigrant ratios (18–21 %) and lower proportions of people in cramped living conditions (6–11 %). The indicators for the remaining six districts were in the middle bracket (Table 1).
Table 1
Number of confirmed SARS-CoV-2 cases per 100 000 inhabitants by district as of 3 December 2020, and selected sociodemographic variables from Oslo City Government’s statistics database.
|
District
|
Confirmed cases per 100 000 inhabitants
|
Proportion of immigrants (%)
|
Mean income (NOK)
|
Proportion in cramped living conditions (%)
|
|
Stovner
|
2 623
|
59.1
|
374 000
|
15.8
|
|
Grorud
|
2 451
|
51.7
|
384 000
|
15.4
|
|
Alna
|
2 380
|
54.7
|
394 000
|
15.4
|
|
Bjerke
|
2 175
|
44.4
|
439 000
|
15.7
|
|
Søndre Nordstrand
|
2 086
|
56.6
|
393 000
|
17.0
|
|
Gamle Oslo
|
1 967
|
39.3
|
446 000
|
11.8
|
|
Grünerløkka
|
1 591
|
34.7
|
451 000
|
11.9
|
|
St. Hanshaugen
|
1 569
|
27.9
|
482 000
|
10.7
|
|
Frogner
|
1 471
|
28.5
|
655 000
|
8.9
|
|
Sagene
|
1 435
|
26.3
|
476 000
|
11.6
|
|
Østensjø
|
1 264
|
26.3
|
489 000
|
10.4
|
|
Nordstrand
|
1 161
|
18.2
|
620 000
|
7.7
|
|
Ullern
|
1 094
|
20.7
|
760 000
|
6.6
|
|
Nordre Aker
|
1 032
|
19.2
|
611 000
|
10.8
|
|
Vestre Aker
|
893
|
17.9
|
817 000
|
6.4
|
Immigrant ratio, socioeconomic status and household density were all independently correlated with infection rates (Figure 1 a–c. Immigrant ratio also had a strong correlation with socioeconomic status and household density with Pearson’s correlation coefficients of −0.916 (95 % CI −0.976 to −0.855) and 0.948 (95 % CI 0.893 to 0.979) respectively, both with p <0.001. Socioeconomic status was negatively correlated to household density with Pearson’s correlation coefficient −0.883 (95 % CI −0.955 to −0.797), p <0.001.
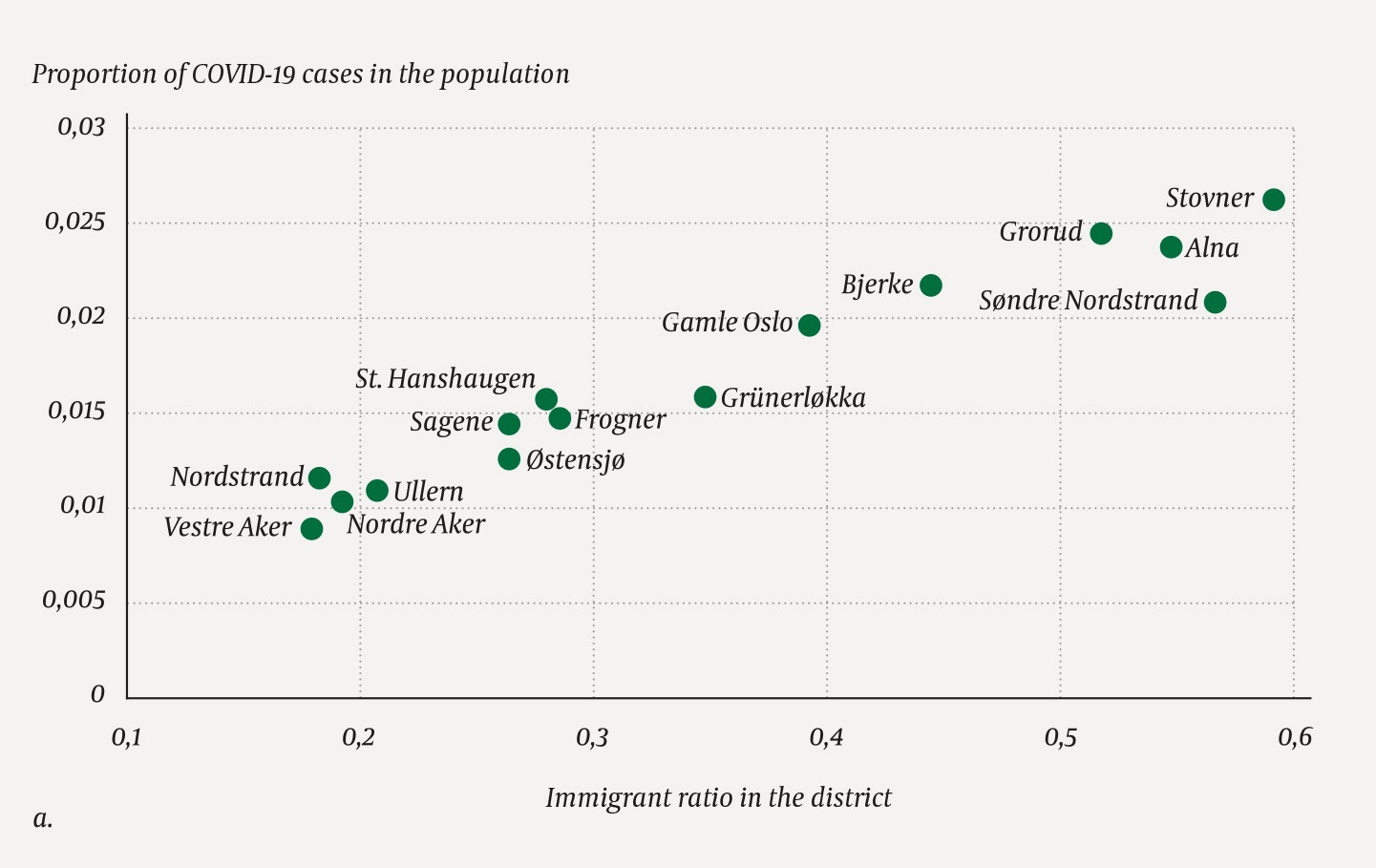
Figure 1a Proportion of confirmed COVID-19 cases per district as of 3 December 2020 by immigrant ratio (Pearson’s correlation coefficient 0.965 (95 % CI 0.925 to 0.992), p <0.001).
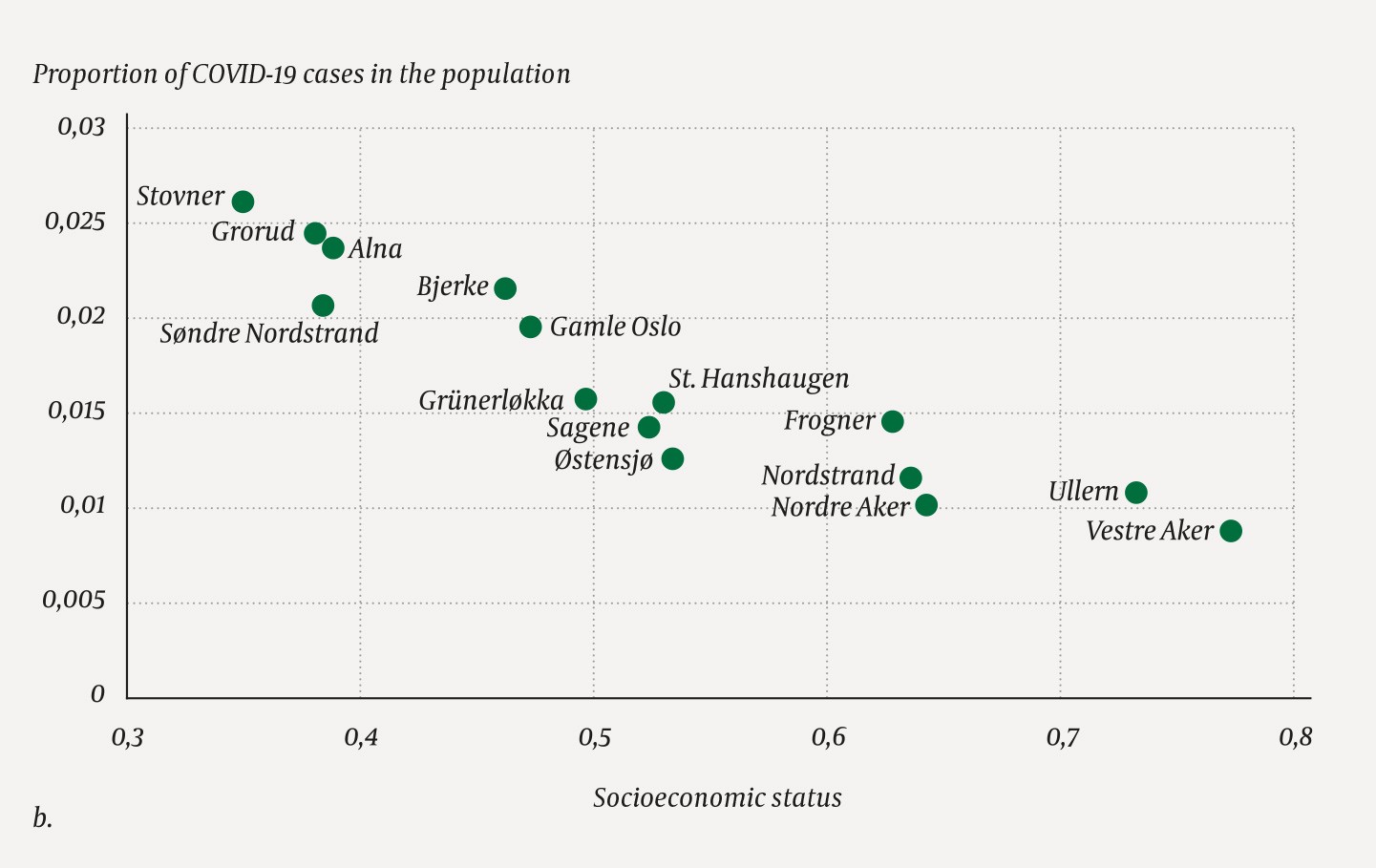
Figure 1b Proportion of confirmed COVID-19 cases per district as of 3 December 2020 by socioeconomic status (Pearson’s correlation coefficient −0.925 (95 % CI −0.967 to −0.862), p <0.001).
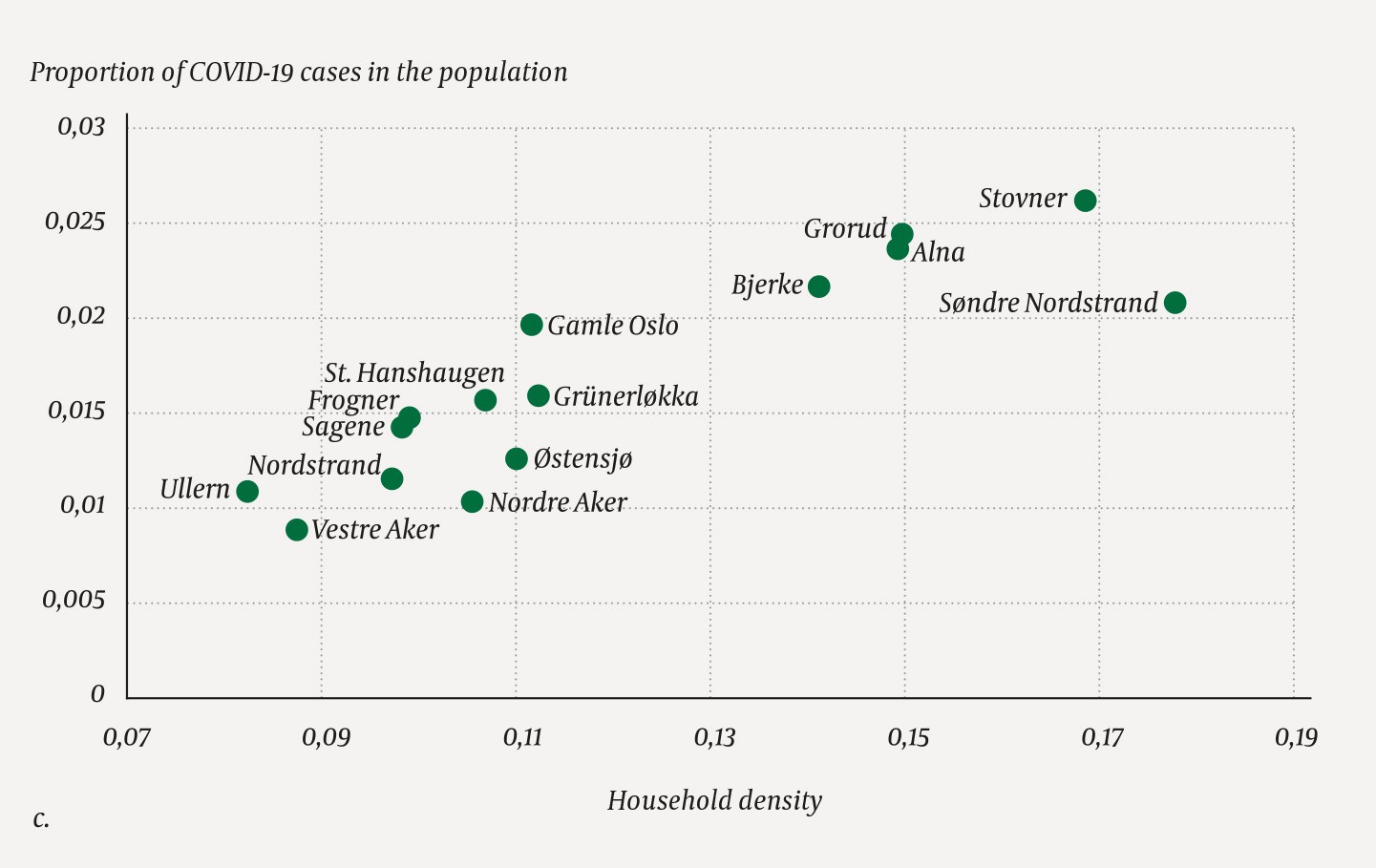
Figure 1c Proportion of confirmed COVID-19 cases per district as of 3 December 2020 by household density (Pearson’s correlation coefficient 0.880 (95 % CI 0.767 to 0.976, p <0.001).
Table 2 shows the results of a regression analysis performed on each of these variables individually as well as a multi-adjusted analysis performed on the three variables simultaneously. In the multi-adjusted analysis, we see that the correlation for immigrant ratio is still statistically significant, while the correlation for socioeconomic status is reduced and non-significant, and the correlation for household density is negative and non-significant.
Table 2
Unadjusted and adjusted regression coefficients from a population-weighted multiple linear regression model between the incidence of PCR-confirmed cases of SARS-CoV-2 in Oslo’s districts cumulatively as of 3 December 2020 and selected sociodemographic variables
|
|
|
|
Confirmed cases of SARS-CoV-2
|
|
|
|
Unadjusted B (95 % CI)
|
P-value
|
Adjusted B (95 % CI)
|
P-value
|
|
Socioeconomic status
|
|
−3.90 (−4.91 to −2.88)
|
< 0.001
|
−1.13 (−2.56 to 0.29)
|
0.107
|
|
Household density
|
|
16.58 (10.79 to 22.38)
|
< 0.001
|
−6.71 (−14.35 to 0.92)
|
0.079
|
|
Immigrant ratio
|
|
3.63 (3.04 to 4.22)
|
< 0.001
|
3.95 (2.16 to 5.73)
|
< 0.001
|
Discussion
We found a statistically significant association between the immigrant ratio in the districts and confirmed cases of SARSCoV-2 in Oslo that persisted when we adjusted for socioeconomic status and household density.
The Norwegian Institute of Public Health’s latest report on the correlation between country of origin and confirmed infections in Oslo found similar results. It showed that the average incidence of infection was almost twice as high among people born abroad as those born in Norway, even when adjusted for gender, age and labour market attachment (7).
The Norwegian Institute of Public Health also found major disparities between different country backgrounds, where the incidence was several times higher among people born in Africa, the Middle East and South Asia than those born in Norway and Western Europe (7). Similarly, a British study found that socioeconomic status could not explain the over-representation of infection in ethnic minorities (8).
It may be that cultural/ethnic background in itself is a factor in the spread of infection. For example, there may be other norms for physical and social proximity, or there may be systematic misunderstandings about infection and infection control measures. Language barriers could also be a factor, particularly among immigrants born abroad.
The methodology and statistical analysis of aggregate averages may potentially represent weaknesses in the study. The analysis does not account for the varying uncertainty for each variable in each district. Furthermore, the values of the composite variables are created constructs. We have also used various indicators where the direction of the correlations may be unclear. See Appendix 1 for our assumptions for directions of the correlations. Since household density was negatively associated with the infection rate when we adjusted for immigrant ratio, the latter may be a confounding variable that affects both risk of infection and living situation. One of the strengths of our analysis is that we have easily and quickly found correlations that can be useful for the health authorities etc., and which can form the basis for a more comprehensive analysis of individual data.
