A man treated for stable Parkinson’s disease for 12 years developed a rapid deterioration of parkinsonian symptoms, mainly presenting as generalised rigidity. The dose of levodopa was increased without effect and upon hospitalisation he could not walk. Increased parkinsonism was found, but no recent neurological outcomes.
A 75-year-old man had been treated for Parkinson’s disease for 12 years and 300 mg levodopa per day had been effective. The disease developed slowly the first years, but after a while his bodily posture changed; thoracic kyphosis increased, his gait became shorter and more dragging, fine motor function was reduced and his arms were less coordinated. In addition he reported a gradually reduced sight. An ophthalmologist performed a perimetric examination, which showed left-sided haemianopsy in the right eye and a generally reduced field of sight on the left eye. No cause was found for the diminishing sight. Contrast- enhanced MR- imaging of the brain showed a few non-specific signal changes as well as a spacious ventricular system.
Parkinson’s disease is a common neurodegenerative disease with a prevalence of 1 % in the population above 65 – 70 years. Loss of dopaminergic neurons in the substantia nigra in the brain stem is a typical neuroanatomical finding. Rest tremor, rigidity, akinesia and balance problems are typical symptoms. The disease tends to start asymmetric and one side of the body usually has more symptoms than the other side (also later in the course of the disease). Patients usually have good use of dopaminergic treatment the first years. If the patient has symmetric disease, autonomous symptoms, cerebral outcomes, dementia, increased reflexes or other pyramidal outcomes, one should consider other reasons for the parkinsonism. Our patient had a course of development compatible with Parkinson’s disease. Narrowed field of sight is uncommon with Parkinson’s disease and that should have triggered us to look for other causes. In this case no cause was found for the problem, and no worsening of sight was reported later.
One year later he developed rigidity in arms and legs during a few weeks. He needed help to dress and undress and was therefore admitted to a nursing home before he consulted a neurologist. A clinical neurological examination revealed marked rigidity axially and in arms and legs. He had difficulty getting up from a chair and walked very slowly and unsteadily. No abnormal reflexes or spasticity were found during the examination. His condition was interpreted as increasing parkinsonism and the levodopa dose was increased to 400 mg per day. However, he became worse with this dose and three weeks later he was admitted to the neurological department. The personnel in the nursing home reported that he had been unable to walk the last two weeks before admission. The man’s regular general practitioner had in the meantime increased the levodopa dose to 600 mg per day without improvement. Upon admission he was tired but opened his eyes when spoken to. He was oriented about time and place. It was difficult to perform an examination of strength, but he managed to sit without support. His reflexes and sensibility results were normal. There were no signs of spasticity or abnormal reflexes at the time of admission or with clinical follow-up examinations during his stay. MR of the brain showed a contrast-filled tumour of 4 × 6 × 4 cm in the right parietal region (fig 1). He was operated and a histopathological examination showed glioblastoma multiforme. The patient died a few weeks later.
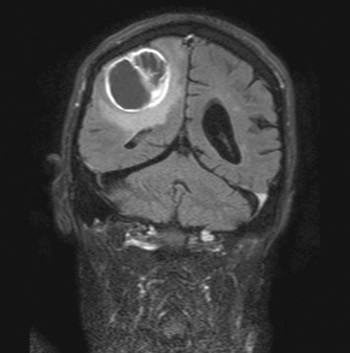
Figure 1 MR of the brain showed 4 × 6 × 4 contrast-filled tumour in the right parietal region. Histological examination showed glioblastoma multiforme
For assessment of muscle tonus the examiner moves the patients’ extremities while the patient relaxes; for patients lying down (conscious or unconscious) tonus can be examined by checking how quickly extremities that have been lifted from the surface fall down again and if there is a difference between sides. A side difference may be an indication of hemiparesis. There are two main types of increased tonus in the muscles; spasticity and rigidity. Spasticity is a consequence of increased reflex activity due to lesions in the upper motor neurons or the corticospinal tracts and can be identified by quick passive movements. Spasticity decreases when the movement is close to the joint’s outer position. Rigidity is a consequence of disease in the basal ganglia (extrapyramidal system) and presents as a coordinated resistance against passive movements irrespective of the joint’s position. If there is a tremor at the same time, one may feel the rigidity as small abrupt movements. This is called «cogh-wheel rigidity».
Glioblastoma multiforme is a high grade infiltrating brain tumour associated with a median survival of about one year. The tumour can grow quickly and is difficult to treat. It is therefore not surprising that the MR examination the year before failed to reveal the tumour.
Discussion
Concomitant disease is known to worsen motoric symptoms in some patients with Parkinson’s disease, but little is known about mechanisms for such interaction. A few cases have been published which indicate that Parkinson symptoms may emerge before tumour specific symptoms (1, 2). Parkinson symptoms secondary to cancer do not improve with drug treatment, but may improve after removal of tumours such as meningomas, acoustic neurinoma or brain metastases (1, 2). Therapy-resistant parkinsonism after radiation therapy of brain tumour has also been described (3).
Our patient had a malignant tumour in the brain and developed sub-acute worsening of pre-existing Parkinson symptoms. Neurological examination with lack of hyperreflexia, spasticity and a positive Babinski’s reflex did not suggest a recent disease in the central nervous system. One may speculate whether spasticity, as well as rigidity was present at the time of the examination. In some cases it may be difficult to separate rigidity and spasticity in a clinical examination and in this case one cannot rule out that there was a comorbid condition. The patient had difficulty walking and problems getting up from a sitting state when examined by a neurologist. These are common symptoms at later stages of Parkinson disease, and the lack of other neurological signs at the examination did not contribute to raising suspicion of other disease. One may later speculate that pareses could have been present and might have been an explanation for the patient’s poor condition.
«Acute akinesia» concomitant with Parkinson disease is defined as sudden worsening of motor functions lasting for more than 24 hours; it may be associated with infections, traumas and disease in the gastrointestinal system (4). Use of medicines is another rare cause for swift onset of parkinsonism. After discontinuing or reducing the intake of dopainergic drugs, some patients may develop sub-acute rigidity; i.e. the Parkinsonism-Hyperpyrexia syndrome. This condition presents in a similar way as Neuroleptic Malignant Syndrome, which is characterised by rigidity, reduced consciousness and autonomous dysfunction, fever, increased values of creatinine kinase and parkinsonian symptoms (5 – 7). Other rare causes for quick development of parkinsonism are vascular lesions in basal ganglia and intoxification with carbon monoxide and methanol. The Serotoninergic syndrome, which may be caused by intake of serotonin reuptake inhibitors and MAO-B inhibitors (seligin), may cause marked rigidity, autonomous dysfunction and mental affection (7, 8).
Conclusion
The medical history describes sub-acute worsening of motor parkinsonian symptoms in a patient who first had a slow disease progression. Doctors who treat patients with Parkinson disease should be aware of acute or sub-acute worsening of motoric functions and maybe especially rigidity, which can be a sign of a tumour in the central nervous system as in our case.
